

Patterns of coronal and sagittal deformities in adolescent idiopathic scoliosis
- PMID: 33419438
- PMCID: PMC7791682
- DOI: 10.1186/s12891-020-03937-4
Patterns of coronal and sagittal deformities in adolescent idiopathic scoliosis
Abstract
Background: Thoracic scoliosis has been shown to be associated with hypokyphosis in adolescent idiopathic scoliosis (AIS). However, the relationship of sagittal spino-pelvic parameters with different coronal curve patterns and their influence on patient-perceived quality of life is unknown. This study aims to determine the association between coronal and sagittal malalignment in patients with AIS and to determine their effects on SRS-22r scores.
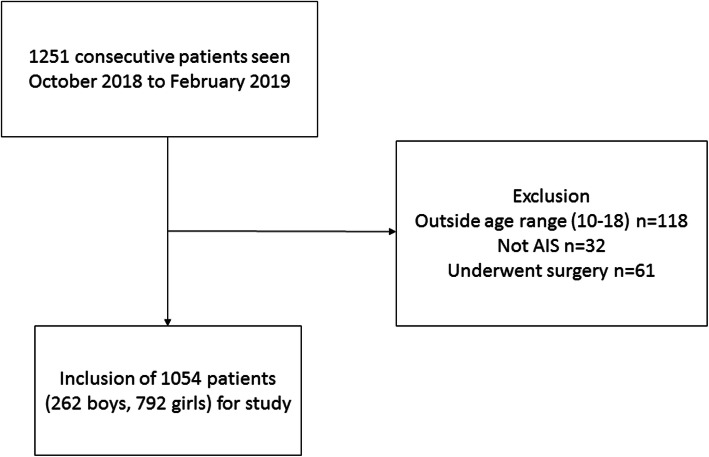
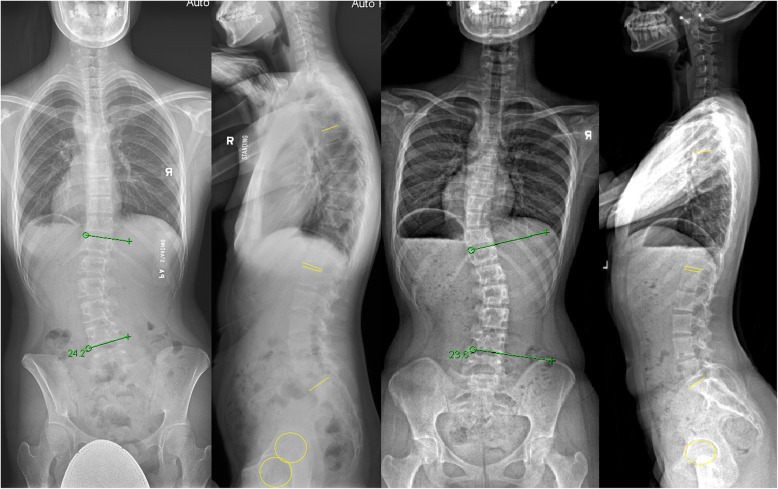
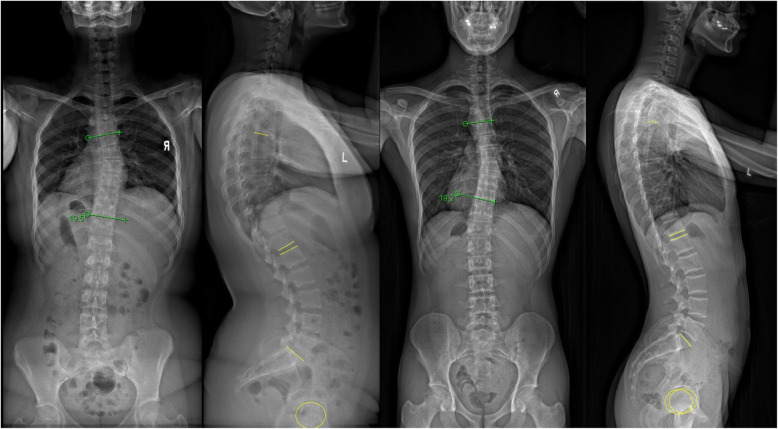
Methods: A cross-sectional study was conducted on 1054 consecutive patients with AIS. The coronal Cobb angle, thoracic kyphosis (TK), lumbar lordosis (LL), pelvic incidence (PI), PI-LL mismatch (PI-LL), pelvic tilt (PT), and sacral slope (SS) were measured on standing radiographs. The coronal Cobb angle (mild: 10-20°; moderate: > 20-40°; severe: > 40°) and PI (low: < 35°; average: 35-50°; high: > 50°) were divided into 3 sub-groups for comparison. Relationship between coronal curve magnitudes and sagittal parameters was studied as was their association with SRS-22r scores.
Results: Low PI had smaller SS (30.1 ± 8.3° vs 44.8 ± 7.7°; p < 0.001), PT (- 0.3 ± 8.1° vs 14.4 ± 7.5°; p < 0.001), and LL (42.0 ± 13.2° vs 55.1 ± 10.6°; p < 0.001), negative PI-LL mismatch (- 12.1 ± 13.1° vs 4.1 ± 10.5°; p < 0.001) as compared to large PI. There were no significant relationships with PI and TK (p = 0.905) or curve magnitude (p = 0.431). No differences in sagittal parameters were observed for mild, moderate or severe coronal Cobb angles. SRS-22r scores only correlated with coronal Cobb angle and larger Cobb angles were negatively correlated with the function, appearance and pain domains.
Conclusions: The sagittal profile for AIS is associated with the pelvic parameters especially PI but not with the coronal curve pattern. All patients have a similar TK regardless of coronal curve type. However, it appears that the coronal deformity is a greater influence on quality of life outcomes especially those > 40°.
Keywords: Adolescent idiopathic scoliosis; Lumbar lordosis; Pelvic incidence; Pelvic tilt; Sacral slope; Thoracic kyphosis.
Conflict of interest statement
There are no financial or non-financial competing interests. JPYC is a senior board member of BMC Musculoskeletal Disorders.
Figures
References
-
- Luk KD, Vidyadhara S, Lu DS, Wong YW, Cheung WY, Cheung KM. Coupling between sagittal and frontal plane deformity correction in idiopathic thoracic scoliosis and its relationship with postoperative sagittal alignment. Spine (Phila Pa 1976) 2010;35(11):1158–1164. - PubMed
-
- Barnes D, Stemper BD, Yogananan N, Baisden JL, Pintar FA. Normal coupling behavior between axial rotation and lateral bending in the lumbar spine - biomed 2009. Biomed Sci Instrum. 2009;45:131–136. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
