

COVID-19: A qualitative chest CT model to identify severe form of the disease
- PMID: 33419693
- PMCID: PMC7746121
- DOI: 10.1016/j.diii.2020.12.002
COVID-19: A qualitative chest CT model to identify severe form of the disease
Abstract
Purpose: The purpose of this study was to identify clinical and chest computed tomography (CT) features associated with a severe form of coronavirus disease 2019 (COVID-19) and to propose a quick and easy to use model to identify patients at risk of a severe form.
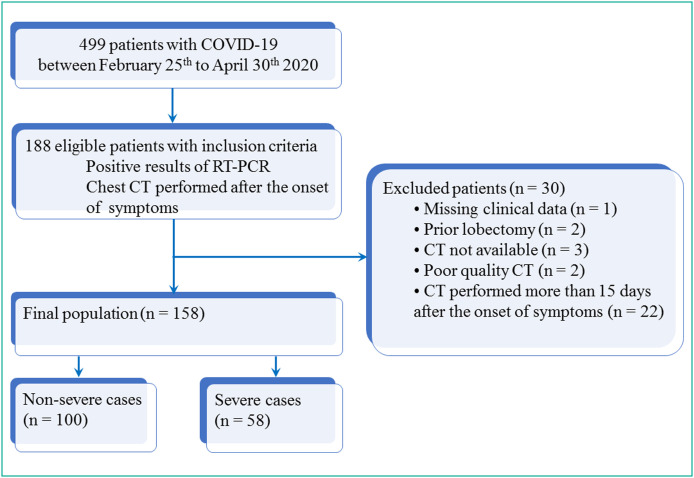
Materials and methods: A total of 158 patients with biologically confirmed COVID-19 who underwent a chest CT after the onset of the symptoms were included. There were 84 men and 74 women with a mean age of 68±14 (SD) years (range: 24-96years). There were 100 non-severe and 58 severe cases. Their clinical data were recorded and the first chest CT examination was reviewed using a computerized standardized report. Univariate and multivariate analyses were performed in order to identify the risk factors associated with disease severity. Two models were built: one was based only on qualitative CT features and the other one included a semi-quantitative total CT score to replace the variable representing the extent of the disease. Areas under the ROC curves (AUC) of the two models were compared with DeLong's method.
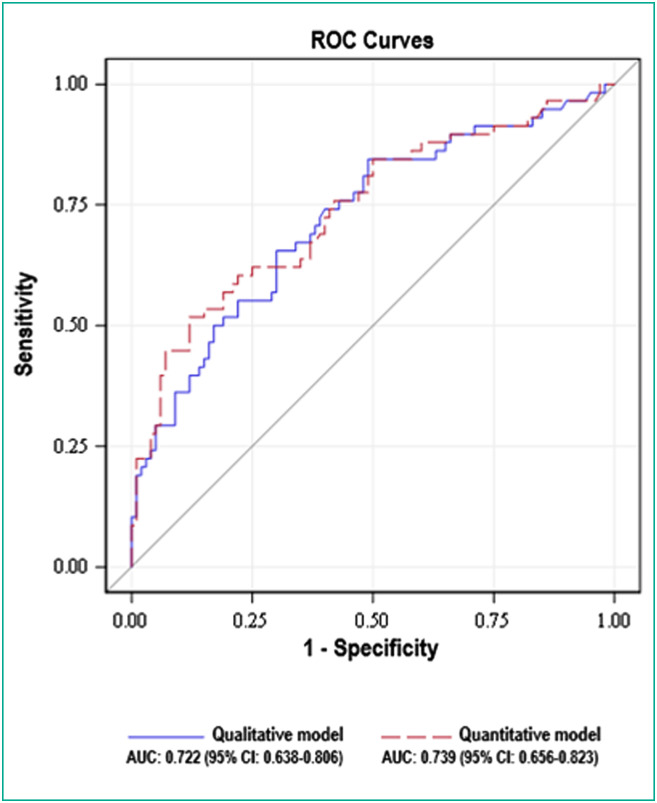
Results: Central involvement of lung parenchyma (P<0.001), area of consolidation (P<0.008), air bronchogram sign (P<0.001), bronchiectasis (P<0.001), traction bronchiectasis (P<0.011), pleural effusion (P<0.026), large involvement of either one of the upper lobes or of the middle lobe (P<0.001) and total CT score≥15 (P<0.001) were more often observed in the severe group than in the non-severe group. No significant differences were found between the qualitative model (large involvement of either upper lobes or middle lobe [odd ratio (OR)=2.473], central involvement [OR=2.760], pleural effusion [OR=2.699]) and the semi-quantitative model (total CT score≥15 [OR=3.342], central involvement [OR=2.344], pleural effusion [OR=2.754]) with AUC of 0.722 (95% CI: 0.638-0.806) vs. 0.739 (95% CI: 0.656-0.823), respectively (P=0.209).
Conclusion: We have developed a new qualitative chest CT-based multivariate model that provides independent risk factors associated with severe form of COVID-19.
Keywords: COVID-19; Risk factors; Severe acute respiratory syndrome coronavirus 2; Severity of illness index; Tomography; X-ray computed (CT).
Copyright © 2020 Société française de radiologie. Published by Elsevier Masson SAS. All rights reserved.
Figures
Similar articles
-
The Performance of Chest CT in Evaluating the Clinical Severity of COVID-19 Pneumonia: Identifying Critical Cases Based on CT Characteristics.Invest Radiol. 2020 Jul;55(7):412-421. doi: 10.1097/RLI.0000000000000689. Invest Radiol. 2020. PMID: 32304402 Free PMC article.
-
Analysis of clinical features and imaging signs of COVID-19 with the assistance of artificial intelligence.Eur Rev Med Pharmacol Sci. 2020 Aug;24(15):8210-8218. doi: 10.26355/eurrev_202008_22510. Eur Rev Med Pharmacol Sci. 2020. PMID: 32767351
-
A new imaging sign in COVID-19 pneumonia: vascular changes and their correlation with clinical severity of the disease.Diagn Interv Radiol. 2021 Mar;27(2):172-180. doi: 10.5152/dir.2020.20346. Diagn Interv Radiol. 2021. PMID: 33044171 Free PMC article.
-
Thoracic imaging tests for the diagnosis of COVID-19.Cochrane Database Syst Rev. 2020 Sep 30;9:CD013639. doi: 10.1002/14651858.CD013639.pub2. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2020 Nov 26;11:CD013639. doi: 10.1002/14651858.CD013639.pub3. PMID: 32997361 Updated.
-
The novel coronavirus pneumonia (COVID-19): a pictorial review of chest CT features.Diagn Interv Radiol. 2021 Mar;27(2):188-194. doi: 10.5152/dir.2020.20304. Diagn Interv Radiol. 2021. PMID: 32815523 Free PMC article. Review.
Cited by
-
COVID-19 pneumonia: The fight must go on.Diagn Interv Imaging. 2021 Feb;102(2):61-62. doi: 10.1016/j.diii.2021.01.006. Diagn Interv Imaging. 2021. PMID: 33494861 Free PMC article. No abstract available.
-
Quantitative Chest CT Analysis: Three Different Approaches to Quantify the Burden of Viral Interstitial Pneumonia Using COVID-19 as a Paradigm.J Clin Med. 2024 Dec 1;13(23):7308. doi: 10.3390/jcm13237308. J Clin Med. 2024. PMID: 39685766 Free PMC article.
-
Imaging of COVID-19: An update of current evidences.Diagn Interv Imaging. 2021 Sep;102(9):493-500. doi: 10.1016/j.diii.2021.05.006. Epub 2021 May 25. Diagn Interv Imaging. 2021. PMID: 34088635 Free PMC article. Review.
-
The Multifaceted COVID-19: CT Aspects of Its Atypical Pulmonary and Abdominal Manifestations and Complications in Adults and Children. A Pictorial Review.Microorganisms. 2021 Sep 26;9(10):2037. doi: 10.3390/microorganisms9102037. Microorganisms. 2021. PMID: 34683358 Free PMC article. Review.
-
Short and Long-Term Impact of COVID-19 Infection on Previous Respiratory Diseases.Arch Bronconeumol. 2022 Apr;58 Suppl 1:39-50. doi: 10.1016/j.arbres.2022.03.011. Epub 2022 Apr 15. Arch Bronconeumol. 2022. PMID: 35501222 Free PMC article. Review.
References
-
- Wu Z., McGoogan J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72,314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020;323:1239–1242. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
