

Pulmonary function and radiological features 4 months after COVID-19: first results from the national prospective observational Swiss COVID-19 lung study
- PMID: 33419891
- PMCID: PMC8082329
- DOI: 10.1183/13993003.03690-2020
Pulmonary function and radiological features 4 months after COVID-19: first results from the national prospective observational Swiss COVID-19 lung study
Abstract
Background: The infectious coronavirus disease 2019 (COVID-19) pandemic is an ongoing global healthcare challenge. Up to one-third of hospitalised patients develop severe pulmonary complications and acute respiratory distress syndrome. Pulmonary outcomes following COVID-19 are unknown.
Methods: The Swiss COVID-19 lung study is a multicentre prospective cohort investigating pulmonary sequelae of COVID-19. We report on initial follow-up 4 months after mild/moderate or severe/critical COVID-19 according to the World Health Organization severity classification.
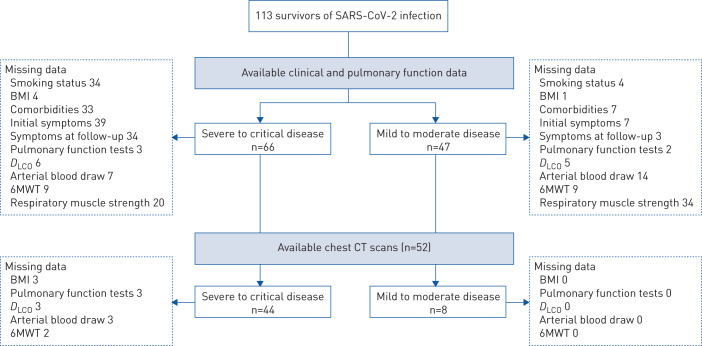
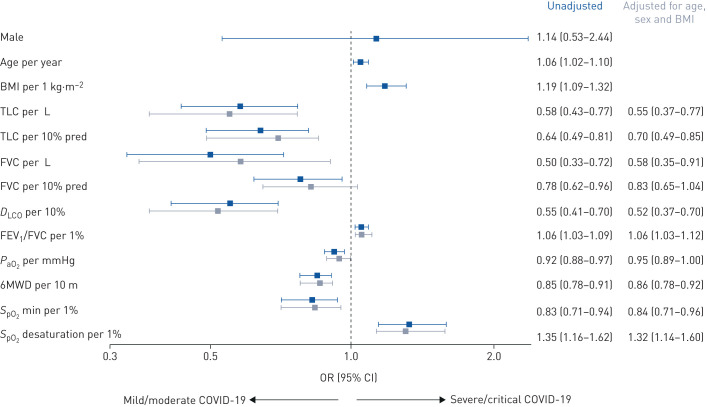
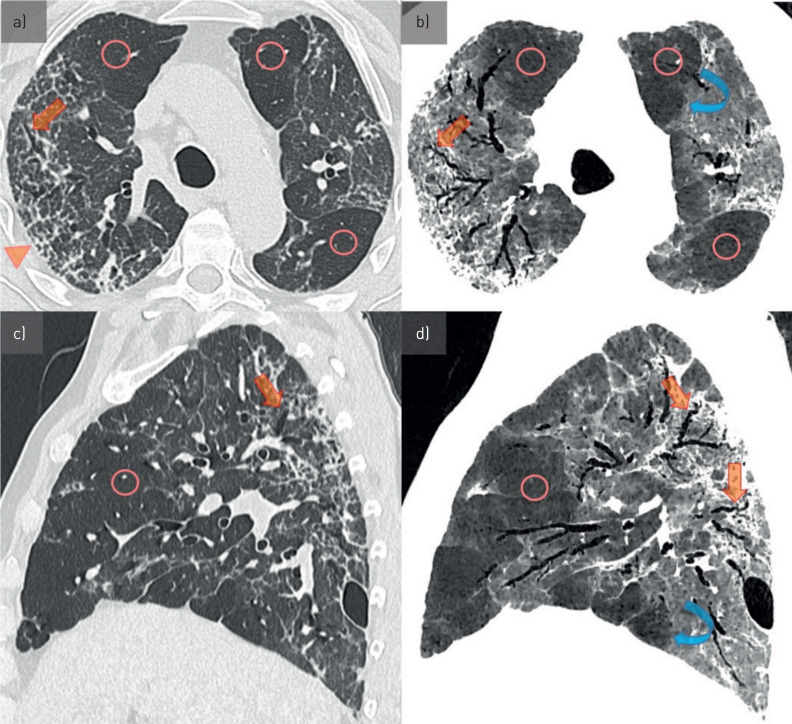
Results: 113 COVID-19 survivors were included (mild/moderate n=47, severe/critical n=66). We confirmed several comorbidities as risk factors for severe/critical disease. Severe/critical disease was associated with impaired pulmonary function, i.e. diffusing capacity of the lung for carbon monoxide (D LCO) % predicted, reduced 6-min walk distance (6MWD) and exercise-induced oxygen desaturation. After adjustment for potential confounding by age, sex and body mass index (BMI), patients after severe/critical COVID-19 had a D LCO 20.9% pred (95% CI 12.4-29.4% pred, p=0.01) lower at follow-up. D LCO % pred was the strongest independent factor associated with previous severe/critical disease when age, sex, BMI, 6MWD and minimal peripheral oxygen saturation at exercise were included in the multivariable model (adjusted odds ratio per 10% predicted 0.59, 95% CI 0. 37-0.87; p=0.01). Mosaic hypoattenuation on chest computed tomography at follow-up was significantly associated with previous severe/critical COVID-19 including adjustment for age and sex (adjusted OR 11.7, 95% CI 1.7-239; p=0.03).
Conclusions: 4 months after severe acute respiratory syndrome coronavirus 2 infection, severe/critical COVID-19 was associated with significant functional and radiological abnormalities, potentially due to small-airway and lung parenchymal disease. A systematic follow-up for survivors needs to be evaluated to optimise care for patients recovering from COVID-19.
Copyright ©ERS 2021.
Conflict of interest statement
Conflict of interest: S.A. Guler has nothing to disclose. Conflict of interest: L. Ebner has nothing to disclose. Conflict of interest: C. Beigelman reports personal fees for lectures from AstraZeneca and Boehringer, outside the submitted work. Conflict of interest: P-O. Bridevaux has nothing to disclose. Conflict of interest: M. Brutsche has nothing to disclose. Conflict of interest: C. Clarenbach reports personal fees from Roche, Novartis, Boehringer, GSK, AstraZeneca, Sanofi, Vifor and Mundipharma, outside the submitted work. Conflict of interest: C. Garzoni has nothing to disclose. Conflict of interest: T.K. Geiser has nothing to disclose. Conflict of interest: A. Lenoir has nothing to disclose. Conflict of interest: M. Mancinetti has nothing to disclose. Conflict of interest: B. Naccini has nothing to disclose. Conflict of interest: S.R. Ott has nothing to disclose. Conflict of interest: L. Piquilloud has nothing to disclose. Conflict of interest: M. Prella has nothing to disclose. Conflict of interest: Y-A. Que has nothing to disclose. Conflict of interest: P.M. Soccal has nothing to disclose. Conflict of interest: C. von Garnier has nothing to disclose. Conflict of interest: M. Funke-Chambour has nothing to disclose.
Figures
Comment in
-
Nefer, Sinuhe and clinical research assessing post COVID-19 condition.Eur Respir J. 2021 Apr 29;57(4):2004423. doi: 10.1183/13993003.04423-2020. Print 2021 Apr. Eur Respir J. 2021. PMID: 33380509 Free PMC article.
-
Pneumopathie interstitielle inflammatoire persistante post Covid-19: bonne réponse à de faibles doses de prednisone.Rev Med Suisse. 2021 Feb 10;17(725):322-323. Rev Med Suisse. 2021. PMID: 33586381 French. No abstract available.
References
-
- World Health Organization (WHO). WHO Coronavirus Disease (COVID-19) Dashboard. covid19.who.int/ Date last accessed: November 25, 2020. Date last updated: November 25, 2020.
-
- Bundesamt für Gesundheit (BAG). Coronavirus: Situation in Switzerland. www.bag.admin.ch/bag/de/home/krankheiten/ausbrueche-epidemien-pandemien/... Date last accessed: November 25, 2020. Date last updated: November 25, 2020.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical