

Performance Characteristics of the Vidas SARS-CoV-2 IgM and IgG Serological Assays
- PMID: 33419947
- PMCID: PMC8092742
- DOI: 10.1128/JCM.02292-20
Performance Characteristics of the Vidas SARS-CoV-2 IgM and IgG Serological Assays
Abstract
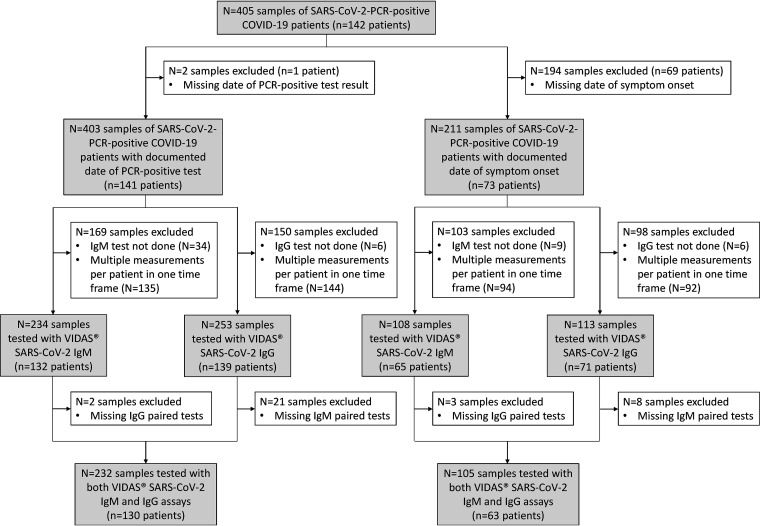
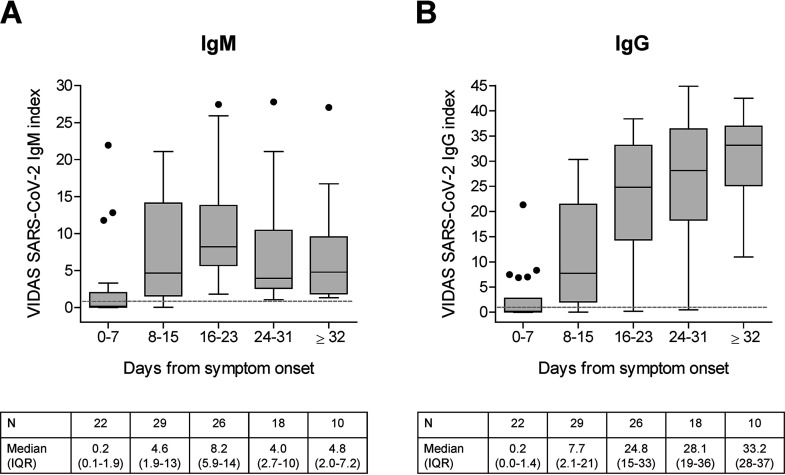
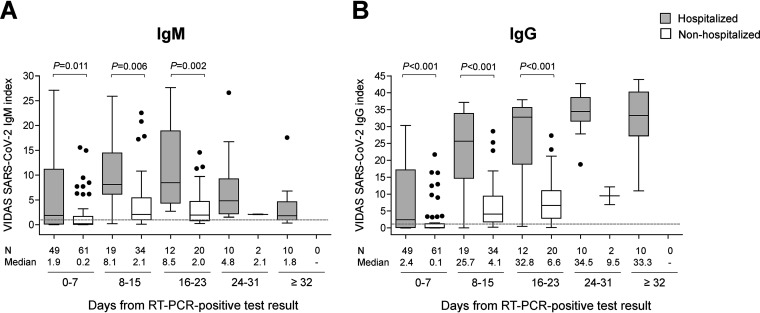
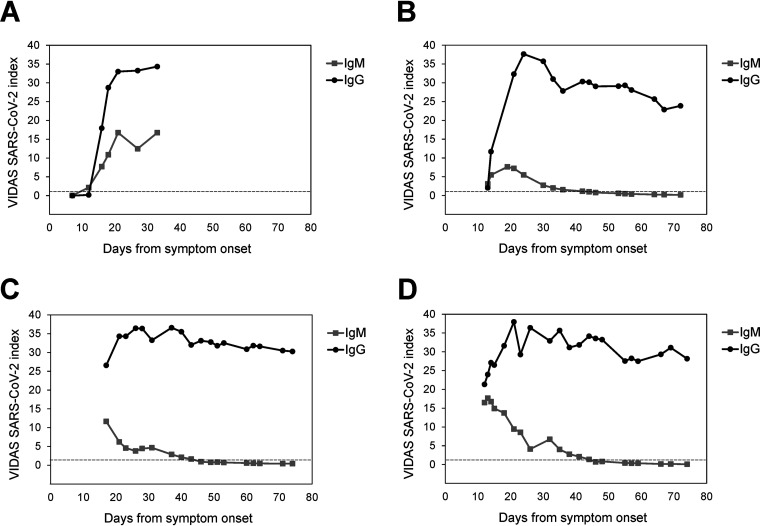
The COVID-19 pandemic, caused by the new severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), continues to spread worldwide. Serological testing for SARS-CoV-2-specific antibodies plays an important role in understanding and controlling the pandemic, notably through epidemiological surveillance. Well-validated and highly specific SARS-CoV-2 serological assays are urgently needed. We describe here the analytical and clinical performance of Vidas SARS-CoV-2 IgM and Vidas SARS-CoV-2 IgG, two CE-marked, emergency use authorization (EUA)-authorized, automated, qualitative assays for the detection of SARS-CoV-2-specific IgM and IgG, respectively. Both assays showed high within-run and within-laboratory precision (coefficients of variation < 11.0%) and very low cross-reactivity toward sera of patients with a past common coronavirus or respiratory virus infection. Clinical specificity determined on up to 989 prepandemic healthy donors was ≥99% with a narrow 95% confidence interval for both IgM and IgG assays. Clinical sensitivity was determined on up to 232 samples from 130 reverse transcriptase PCR (RT-PCR)-confirmed SARS-CoV-2 patients. The positive percent agreement (PPA) with SARS-CoV-2 PCR reached 100% at ≥16 days (Vidas SARS-CoV-2 IgM) and ≥32 days (Vidas SARS-CoV-2 IgG) of symptom onset. Combined IgM/IgG test results improved the PPA compared to each test alone. SARS-CoV-2 IgG seroconversion followed closely that of SARS-CoV-2 IgM and remained stable over time, while SARS-CoV-2 IgM levels rapidly declined. Interestingly, SARS-CoV-2-specific IgM and IgG responses were significantly higher in COVID-19 hospitalized versus nonhospitalized patients. Altogether, the Vidas SARS-CoV-2 IgM and IgG assays are highly specific and sensitive serological tests suitable for the reliable detection of past acute SARS-CoV-2 infections.
Keywords: COVID-19; SARS-CoV-2; Vidas; diagnosis; immunoserology.
Copyright © 2021 Renard et al.
Figures
References
-
- Zhou P, Yang X-L, Wang X-G, Hu B, Zhang L, Zhang W, Si H-R, Zhu Y, Li B, Huang C-L, Chen H-D, Chen J, Luo Y, Guo H, Jiang R-D, Liu M-Q, Chen Y, Shen X-R, Wang X, Zheng X-S, Zhao K, Chen Q-J, Deng F, Liu L-L, Yan B, Zhan F-X, Wang Y-Y, Xiao G-F, Shi Z-L. 2020. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 579:270–273. doi: 10.1038/s41586-020-2012-7. - DOI - PMC - PubMed
-
- World Health Organization. 2020. Coronavirus disease (COVID-19) situation reports. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situatio.... Accessed 29 October 2020.
-
- Johns Hopkins University. 2020. COVID-19 Resource Center. https://coronavirus.jhu.edu/map.html. Accessed 29 October 2020.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
