

Disease risk scores for skin cancers
- PMID: 33420020
- PMCID: PMC7794415
- DOI: 10.1038/s41467-020-20246-5
Disease risk scores for skin cancers
Abstract
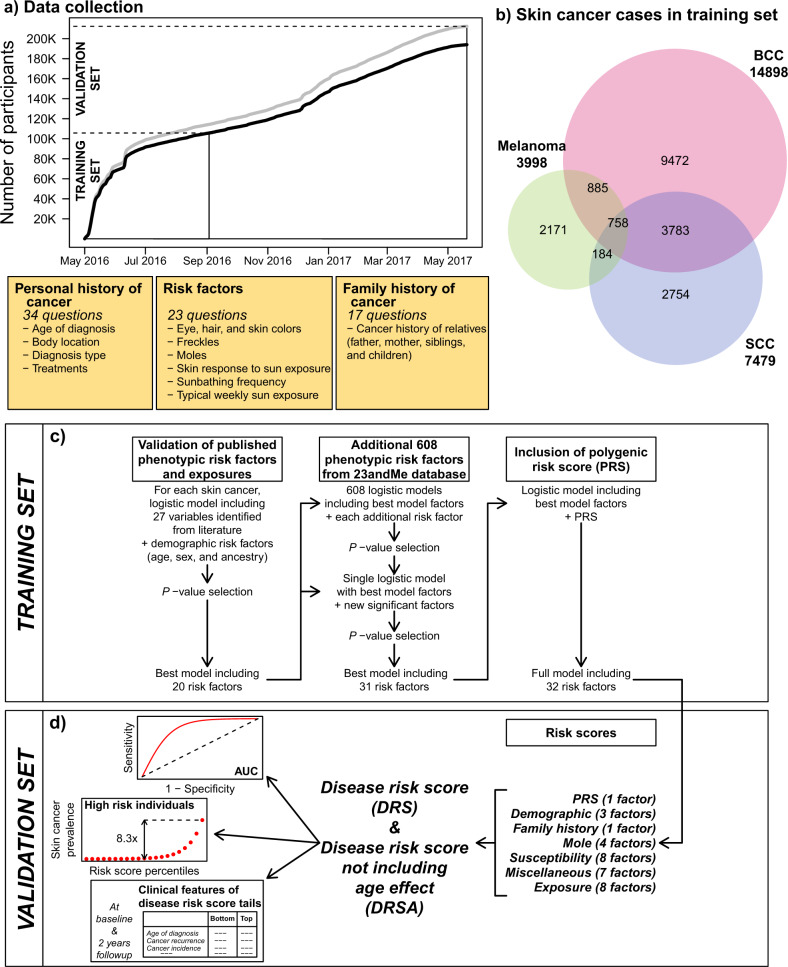
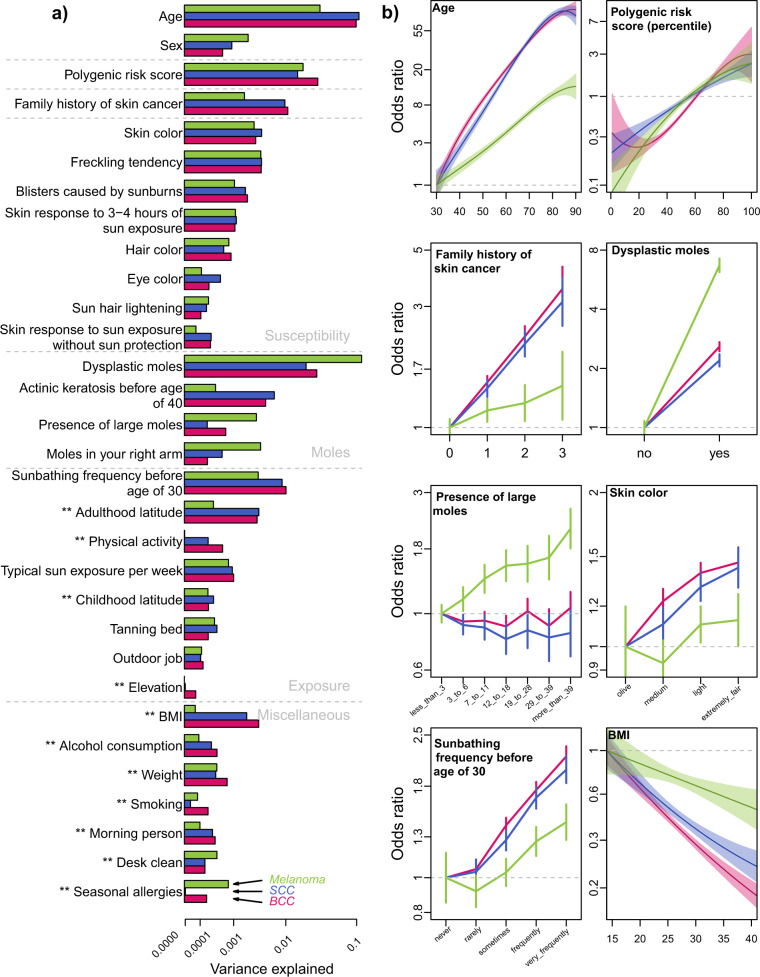
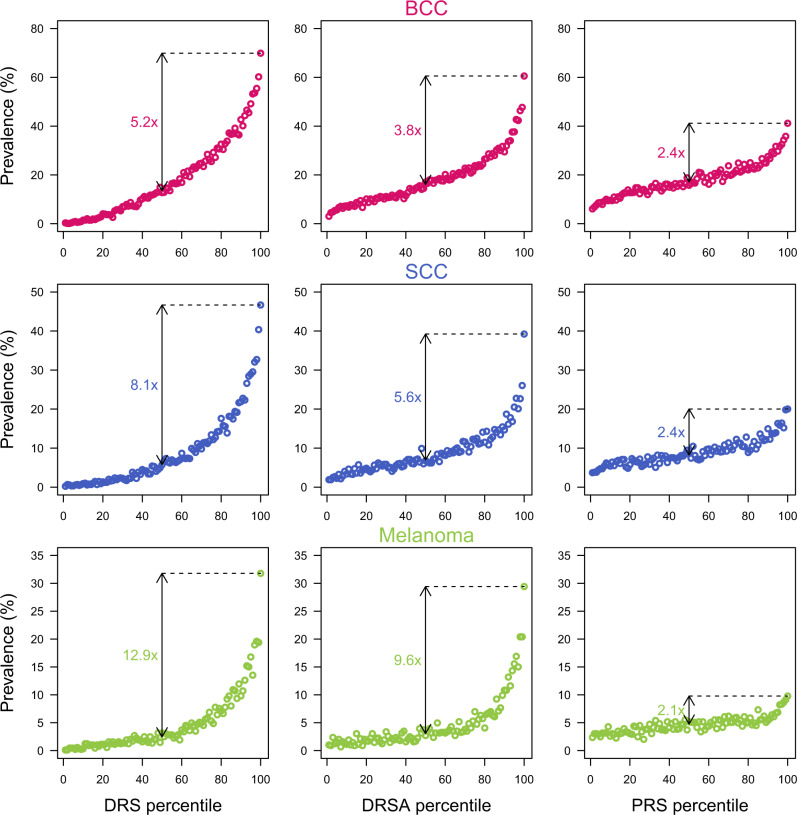
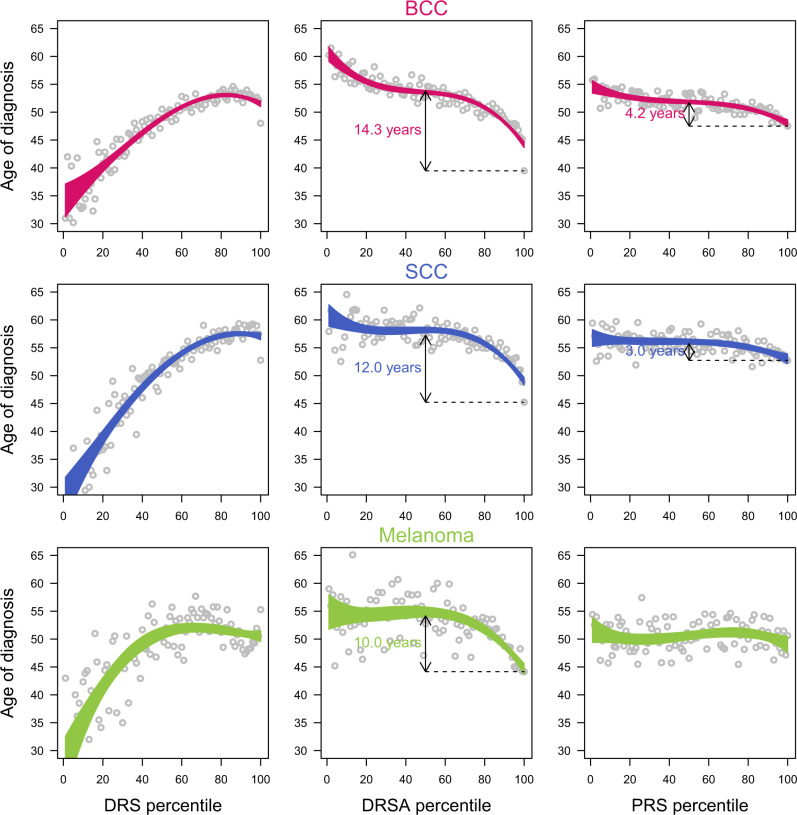
We trained and validated risk prediction models for the three major types of skin cancer- basal cell carcinoma (BCC), squamous cell carcinoma (SCC), and melanoma-on a cross-sectional and longitudinal dataset of 210,000 consented research participants who responded to an online survey covering personal and family history of skin cancer, skin susceptibility, and UV exposure. We developed a primary disease risk score (DRS) that combined all 32 identified genetic and non-genetic risk factors. Top percentile DRS was associated with an up to 13-fold increase (odds ratio per standard deviation increase >2.5) in the risk of developing skin cancer relative to the middle DRS percentile. To derive lifetime risk trajectories for the three skin cancers, we developed a second and age independent disease score, called DRSA. Using incident cases, we demonstrated that DRSA could be used in early detection programs for identifying high risk asymptotic individuals, and predicting when they are likely to develop skin cancer. High DRSA scores were not only associated with earlier disease diagnosis (by up to 14 years), but also with more severe and recurrent forms of skin cancer.
Conflict of interest statement
All authors are current or former employees of 23andMe, Inc., and hold stock or stock options in 23andMe.
Figures

References
-
- World Health Organization. Guide to cancer early diagnosis. World Health Organization; https://apps.who.int/iris/handle/10665/254500 (2017).
-
- Rebbeck TR, et al. Precision prevention and early detection of cancer: fundamental principles. Cancer Discov. 2018;8:803–811. doi: 10.1158/2159-8290.CD-17-1415. - DOI - PubMed
-
- American Cancer Society. Cancer facts & figures 2019 (American Cancer Society, Atlanta, 2019).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
