

Predicting postoperative peritoneal metastasis in gastric cancer with serosal invasion using a collagen nomogram
- PMID: 33420057
- PMCID: PMC7794254
- DOI: 10.1038/s41467-020-20429-0
Predicting postoperative peritoneal metastasis in gastric cancer with serosal invasion using a collagen nomogram
Abstract
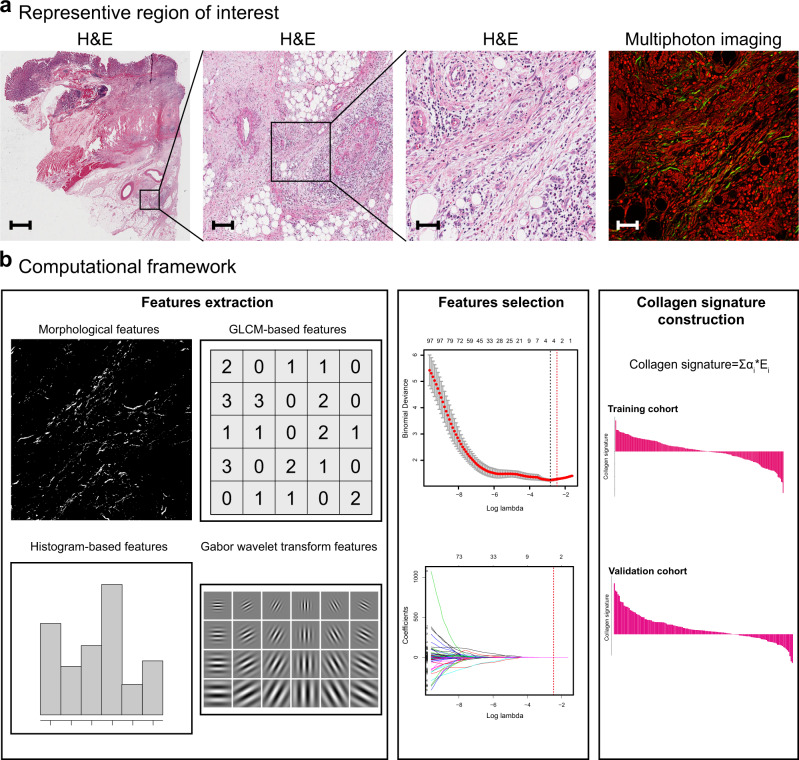
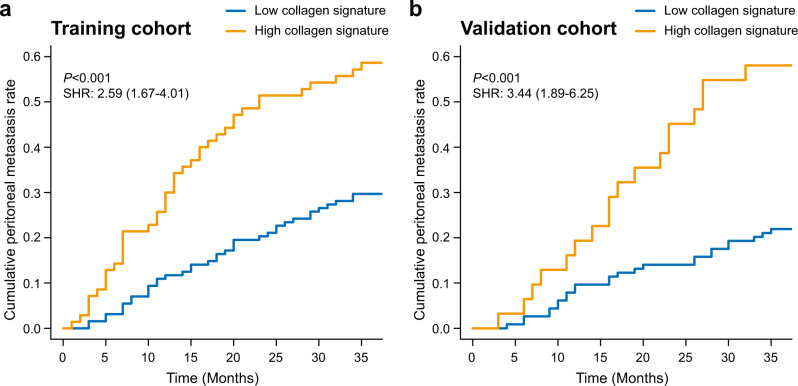
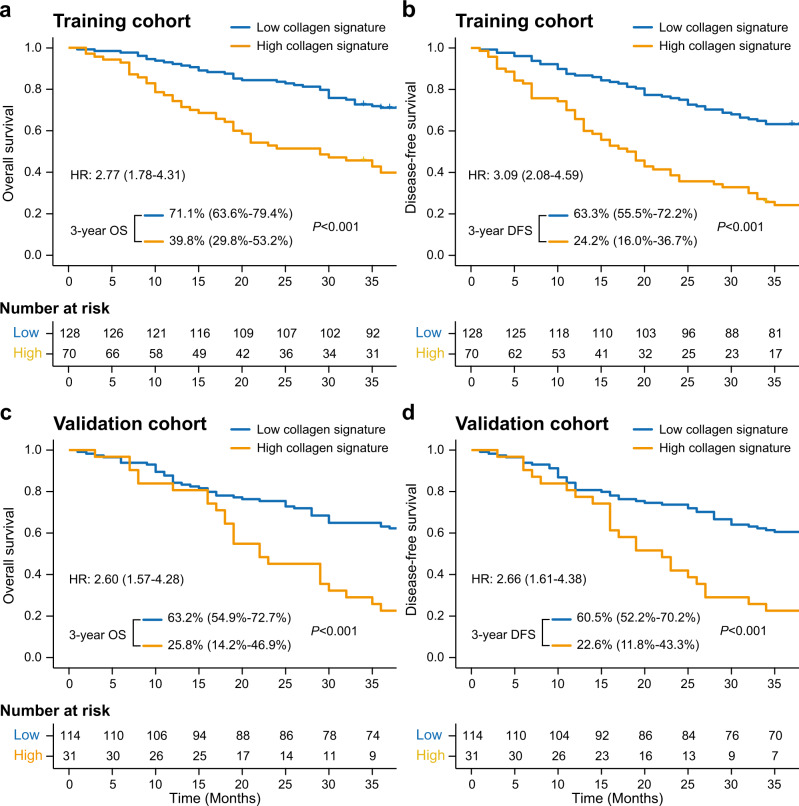
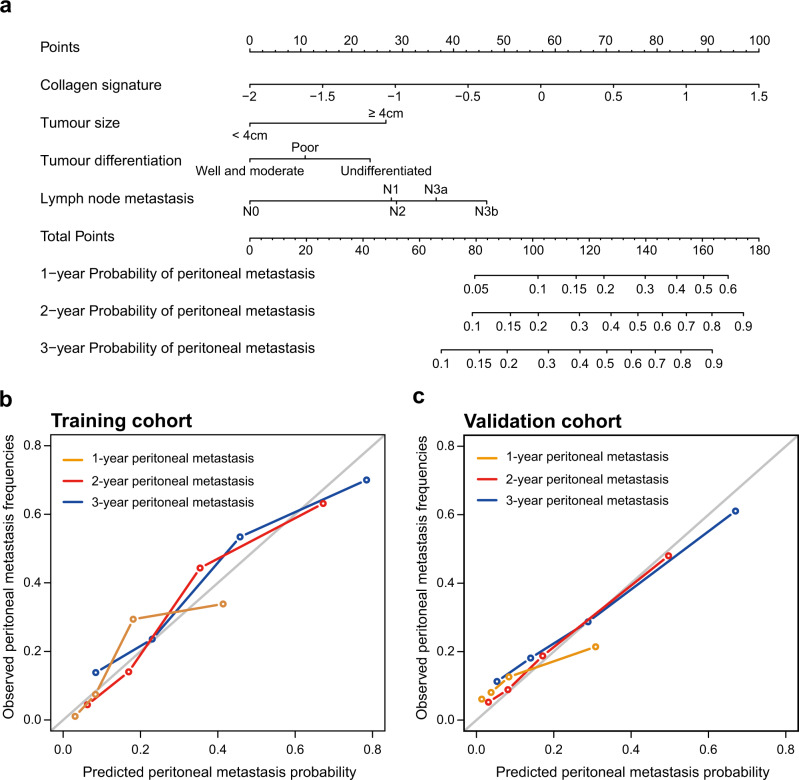
Accurate prediction of peritoneal metastasis for gastric cancer (GC) with serosal invasion is crucial in clinic. The presence of collagen in the tumour microenvironment affects the metastasis of cancer cells. Herein, we propose a collagen signature, which is composed of multiple collagen features in the tumour microenvironment of the serosa derived from multiphoton imaging, to describe the extent of collagen alterations. We find that a high collagen signature is significantly associated with a high risk of peritoneal metastasis (P < 0.001). A competing-risk nomogram including the collagen signature, tumour size, tumour differentiation status and lymph node metastasis is constructed. The nomogram demonstrates satisfactory discrimination and calibration. Thus, the collagen signature in the tumour microenvironment of the gastric serosa is associated with peritoneal metastasis in GC with serosal invasion, and the nomogram can be conveniently used to individually predict the risk of peritoneal metastasis in GC with serosal invasion after radical surgery.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
