

Plasma ctDNA is a tumor tissue surrogate and enables clinical-genomic stratification of metastatic bladder cancer
- PMID: 33420073
- PMCID: PMC7794518
- DOI: 10.1038/s41467-020-20493-6
Plasma ctDNA is a tumor tissue surrogate and enables clinical-genomic stratification of metastatic bladder cancer
Abstract
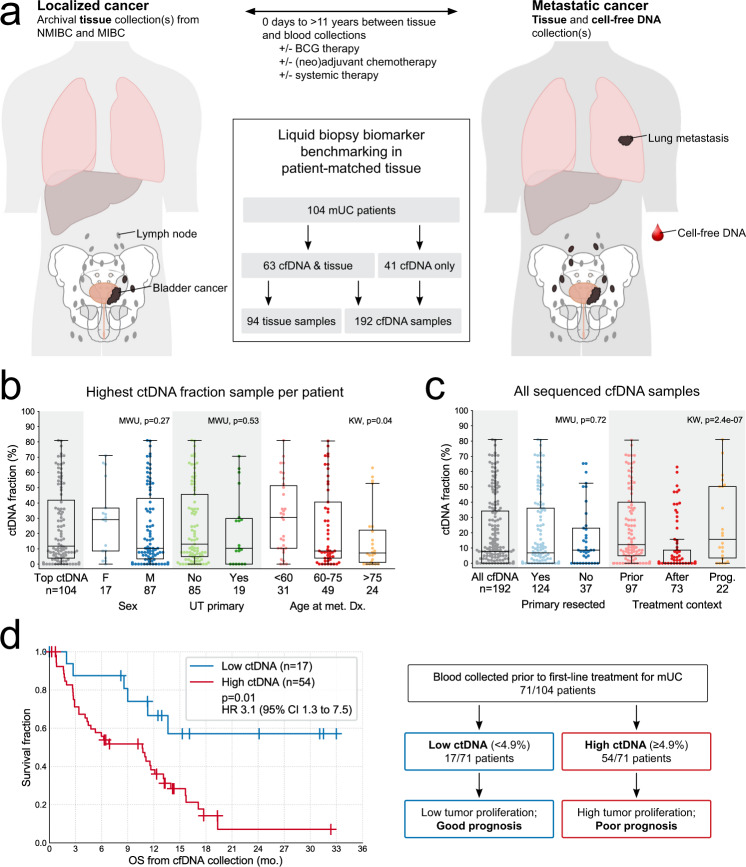
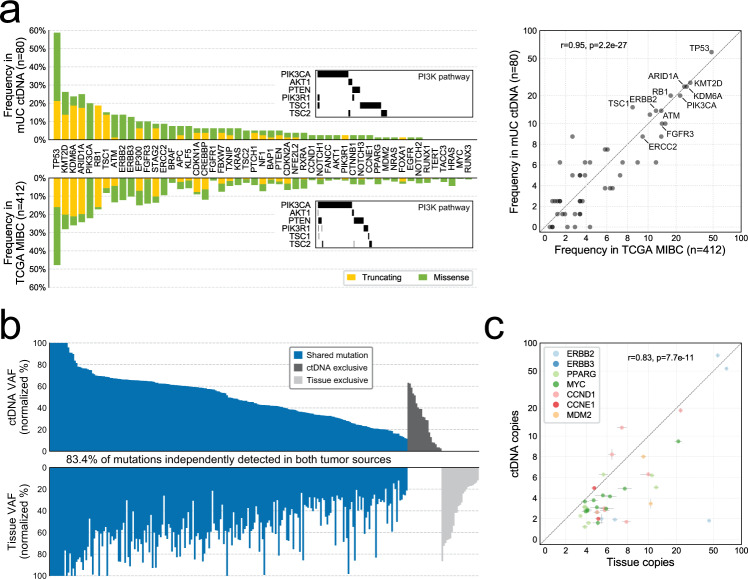
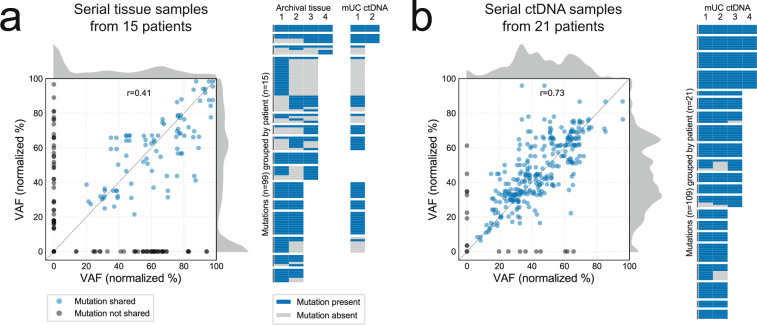
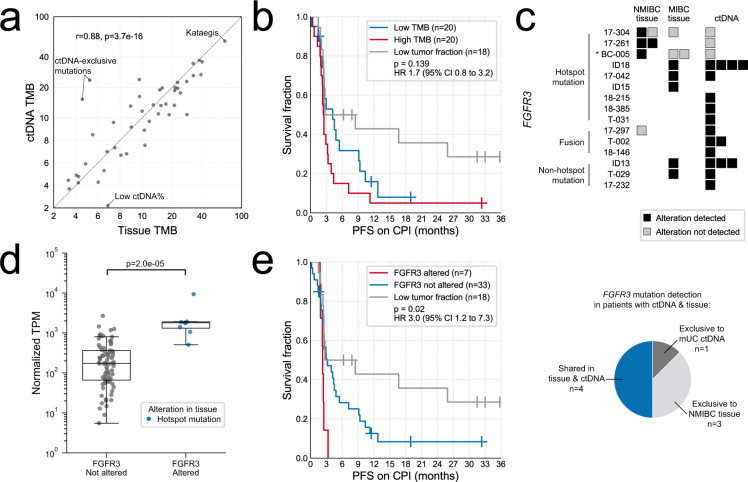
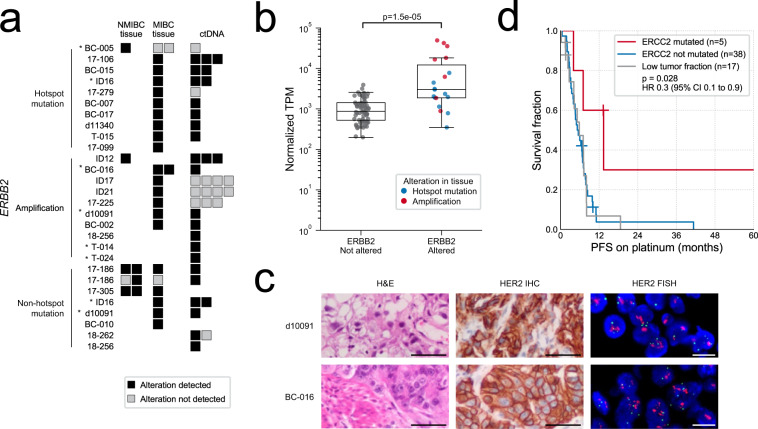
Molecular stratification can improve the management of advanced cancers, but requires relevant tumor samples. Metastatic urothelial carcinoma (mUC) is poised to benefit given a recent expansion of treatment options and its high genomic heterogeneity. We profile minimally-invasive plasma circulating tumor DNA (ctDNA) samples from 104 mUC patients, and compare to same-patient tumor tissue obtained during invasive surgery. Patient ctDNA abundance is independently prognostic for overall survival in patients initiating first-line systemic therapy. Importantly, ctDNA analysis reproduces the somatic driver genome as described from tissue-based cohorts. Furthermore, mutation concordance between ctDNA and matched tumor tissue is 83.4%, enabling benchmarking of proposed clinical biomarkers. While 90% of mutations are identified across serial ctDNA samples, concordance for serial tumor tissue is significantly lower. Overall, our exploratory analysis demonstrates that genomic profiling of ctDNA in mUC is reliable and practical, and mitigates against disease undersampling inherent to studying archival primary tumor foci. We urge the incorporation of cell-free DNA profiling into molecularly-guided clinical trials for mUC.
Conflict of interest statement
J.-M.L. reports honoraria from Pfizer, Astellas, and Ipsen. N.S. reports travel grants from Bayer, MSD, Bristol-Myers Squibb, and Astellas. T.T. reports speaker/consultant roles with Astellas, AstraZeneca, Bayer, BMS, Ipsen, Janssen, MSD, Roche, and Sanofi. E.A.G. is an employee of Decipher Biosciences, Inc. K.N.C. reports receiving commercial research grants and honorarium from Astellas, AstraZeneca, Constellation Pharmaceuticals, Daiichi Sankyo, Janssen, Merck, Novartis, Pfizer, Point Biopharma, Roche, and Sanofi. A.W.W. reports receiving a commercial research grant from Janssen, and honorarium from AstraZeneca, Astellas, Janssen, and Merck. The remaining authors declare no competing interests.
Figures
Comment in
-
Urological Oncology: Bladder, Penis and Urethral Cancer, and Basic Principles of Oncology.J Urol. 2021 Sep;206(3):769-772. doi: 10.1097/JU.0000000000001908. Epub 2021 Jun 16. J Urol. 2021. PMID: 34130485 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
