

Additional SNPs improve risk stratification of a polygenic hazard score for prostate cancer
- PMID: 33420416
- PMCID: PMC8157993
- DOI: 10.1038/s41391-020-00311-2
Additional SNPs improve risk stratification of a polygenic hazard score for prostate cancer
Abstract
Background: Polygenic hazard scores (PHS) can identify individuals with increased risk of prostate cancer. We estimated the benefit of additional SNPs on performance of a previously validated PHS (PHS46).
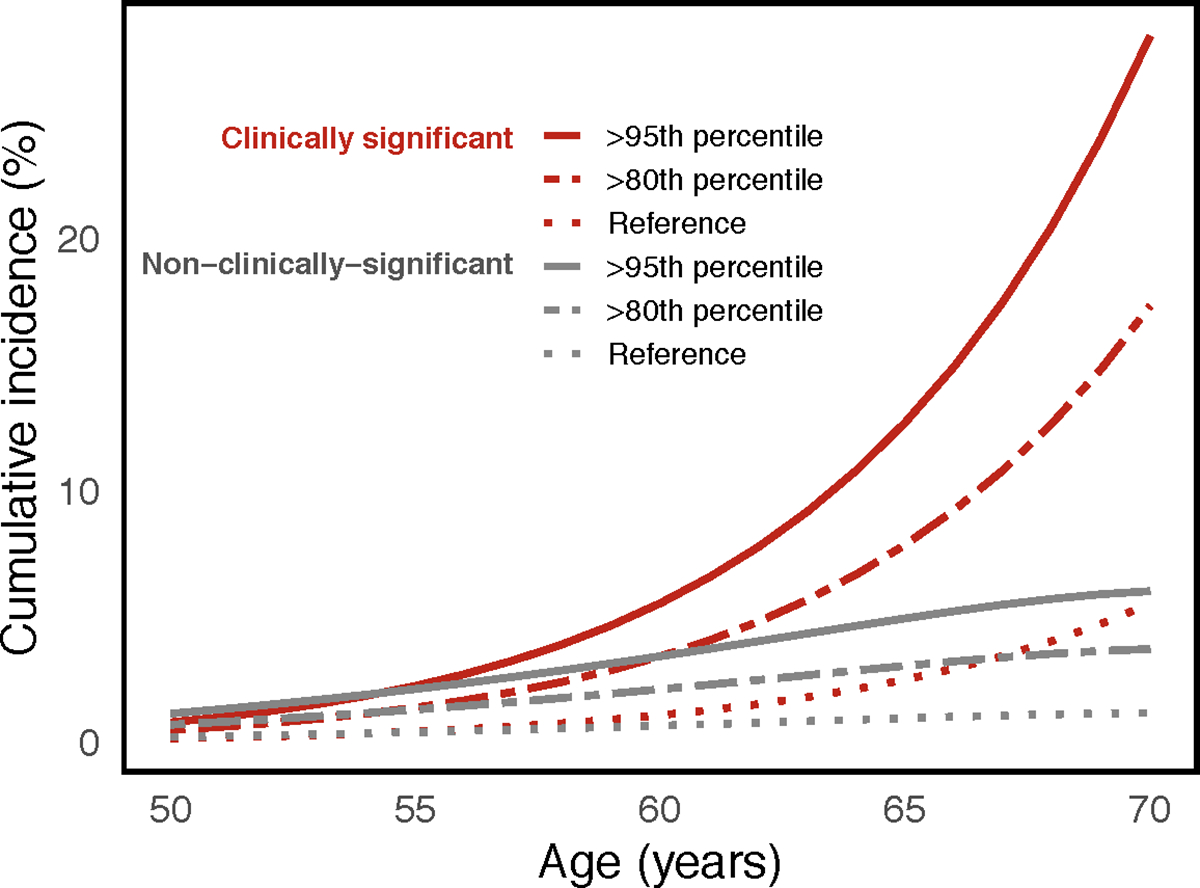
Materials and method: 180 SNPs, shown to be previously associated with prostate cancer, were used to develop a PHS model in men with European ancestry. A machine-learning approach, LASSO-regularized Cox regression, was used to select SNPs and to estimate their coefficients in the training set (75,596 men). Performance of the resulting model was evaluated in the testing/validation set (6,411 men) with two metrics: (1) hazard ratios (HRs) and (2) positive predictive value (PPV) of prostate-specific antigen (PSA) testing. HRs were estimated between individuals with PHS in the top 5% to those in the middle 40% (HR95/50), top 20% to bottom 20% (HR80/20), and bottom 20% to middle 40% (HR20/50). PPV was calculated for the top 20% (PPV80) and top 5% (PPV95) of PHS as the fraction of individuals with elevated PSA that were diagnosed with clinically significant prostate cancer on biopsy.
Results: 166 SNPs had non-zero coefficients in the Cox model (PHS166). All HR metrics showed significant improvements for PHS166 compared to PHS46: HR95/50 increased from 3.72 to 5.09, HR80/20 increased from 6.12 to 9.45, and HR20/50 decreased from 0.41 to 0.34. By contrast, no significant differences were observed in PPV of PSA testing for clinically significant prostate cancer.
Conclusions: Incorporating 120 additional SNPs (PHS166 vs PHS46) significantly improved HRs for prostate cancer, while PPV of PSA testing remained the same.
Figures
References
-
- Witte JS. Personalized prostate cancer screening: Improving PSA tests with genomic information. Sci Transl Med 2010; 2: 1–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
