

Closing the Osteoporosis Care Gap
- PMID: 33420632
- PMCID: PMC7935825
- DOI: 10.1007/s11914-020-00644-w
Closing the Osteoporosis Care Gap
Abstract
Purpose of review: This review outlines the scope of the problem in osteoporosis care and secondary fracture prevention and describes fracture prevention strategies, with a focus on the frail elderly.
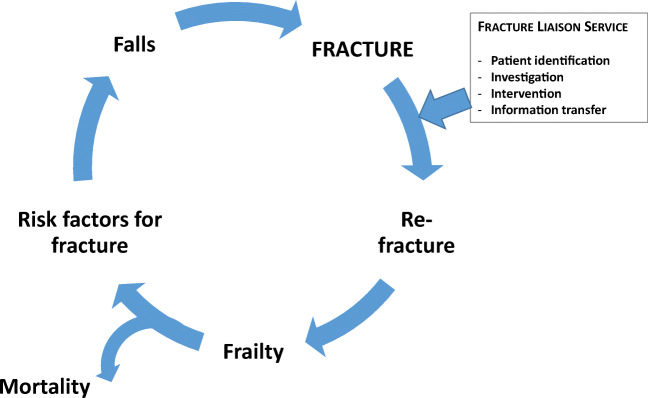
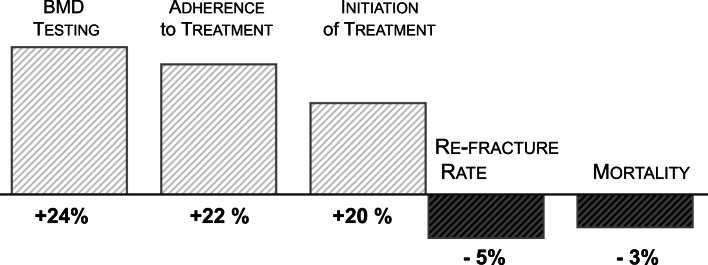
Recent findings: Despite heightened awareness among patients and clinicians alike and the availability of efficacious anti-osteoporosis medications, osteoporosis is still underdiagnosed and undertreated. However, the introduction of systematic risk assessment and secondary fracture prevention programmes has gained momentum, and evidence of success is accumulating. We possess today the knowledge required to close the osteoporosis care gap. The basic components in a secondary prevention model are similar in all health care settings, number one being a dedicated fracture coordinator, with anti-osteoporosis medications and multifaceted falls prevention as cornerstones, particularly in the frailest, both in the near and long-term. Initiation of structured care pathways including the key elements - identification, investigation, intervention and follow-up of adherence - demonstrably reduces re-fracture rates and is cost-effective.
Keywords: Elderly; Fracture; Fracture liaison service; Frailty; Prevention.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Klotzbuecher CM, Ross PD, Landsman PB, Abbott TA, 3rd, Berger M. Patients with prior fractures have an increased risk of future fractures: a summary of the literature and statistical synthesis. J Bone Miner Res. 2000;15(4):721–739. - PubMed
-
- Kanis JA, Johnell O, De Laet C, Johansson H, Oden A, Delmas P, et al. A meta-analysis of previous fracture and subsequent fracture risk. Bone. 2004;35(2):375–382. - PubMed
-
- Johansson H, Oden A, McCloskey EV, Kanis JA. Mild morphometric vertebral fractures predict vertebral fractures but not non-vertebral fractures. Osteoporos Int. 2014;25(1):235–241. - PubMed
-
- Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 2006;17(12):1726–1733. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
