

COVID-19: Neuroimaging Features of a Pandemic
- PMID: 33421032
- PMCID: PMC8014046
- DOI: 10.1111/jon.12819
COVID-19: Neuroimaging Features of a Pandemic
Abstract
Background and purpose: The ongoing Coronavirus Disease 2019 (COVID-19) pandemic is caused by the novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). COVID-19 is occasionally associated with manifold diseases of the central nervous system (CNS). We sought to present the neuroimaging features of such CNS involvement. In addition, we sought to identify typical neuroimaging patterns that could indicate possible COVID-19-associated neurological manifestations.
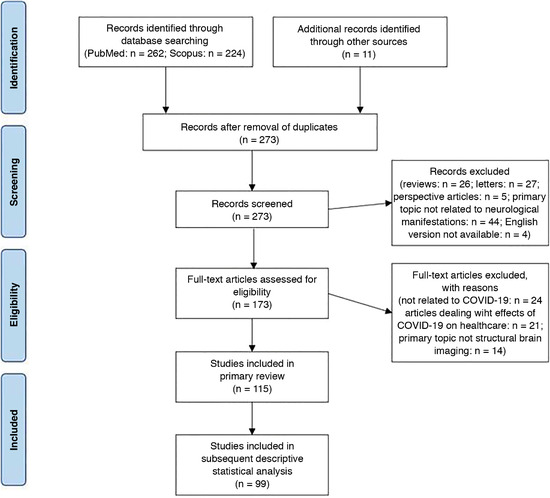
Methods: In this systematic literature review, typical neuroimaging features of cerebrovascular diseases and inflammatory processes associated with COVID-19 were analyzed. Reports presenting individual patient data were included in further quantitative analysis with descriptive statistics.
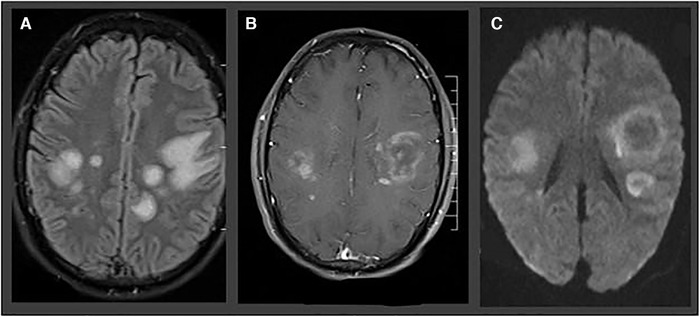
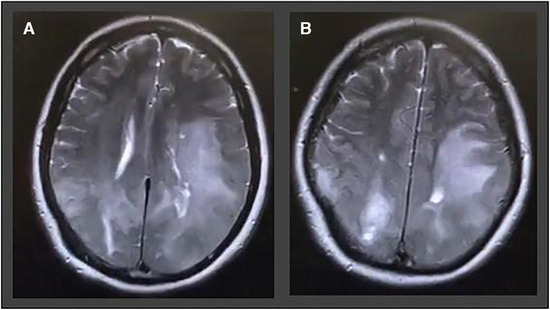
Results: We identified 115 studies reporting a total of 954 COVID-19 patients with associated neurological manifestations and neuroimaging alterations. A total of 95 (82.6%) of the identified studies were single case reports or case series, whereas 660 (69.2%) of the reported cases included individual information and were thus included in descriptive statistical analysis. Ischemia with neuroimaging patterns of large vessel occlusion event was revealed in 59.9% of ischemic stroke patients, whereas 69.2% of patients with intracerebral hemorrhage exhibited bleeding in a location that was not associated with hypertension. Callosal and/or juxtacortical location was identified in 58.7% of cerebral microbleed positive images. Features of hemorrhagic necrotizing encephalitis were detected in 28.8% of patients with meningo-/encephalitis.
Conclusions: Manifold CNS involvement is increasingly reported in COVID-19 patients. Typical and atypical neuroimaging features have been observed in some disease entities, so that familiarity with these imaging patterns appears reasonable and may assist clinicians in the differential diagnosis of COVID-19 CNS manifestations.
Keywords: COVID-19; CT; MRI; SARS-CoV-2; neuroimaging.
© 2021 The Authors. Journal of Neuroimaging published by Wiley Periodicals LLC on behalf of American Society of Neuroimaging.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
