

Anti-β2-glycoprotein I and anti-prothrombin antibodies cause lupus anticoagulant through different mechanisms of action
- PMID: 33421291
- PMCID: PMC8048633
- DOI: 10.1111/jth.15241
Anti-β2-glycoprotein I and anti-prothrombin antibodies cause lupus anticoagulant through different mechanisms of action
Abstract
Background: The presence of lupus anticoagulant (LA) is an independent risk factor for thrombosis. This laboratory phenomenon is detected as a phospholipid-dependent prolongation of the clotting time and is caused by autoantibodies against beta2-glycoprotein I (β2GPI) or prothrombin. How these autoantibodies cause LA is unclear.
Objective: To elucidate how anti-β2GPI and anti-prothrombin antibodies cause the LA phenomenon.
Methods: The effects of monoclonal anti-β2GPI and anti-prothrombin antibodies on coagulation were analyzed in plasma and with purified coagulation factors.
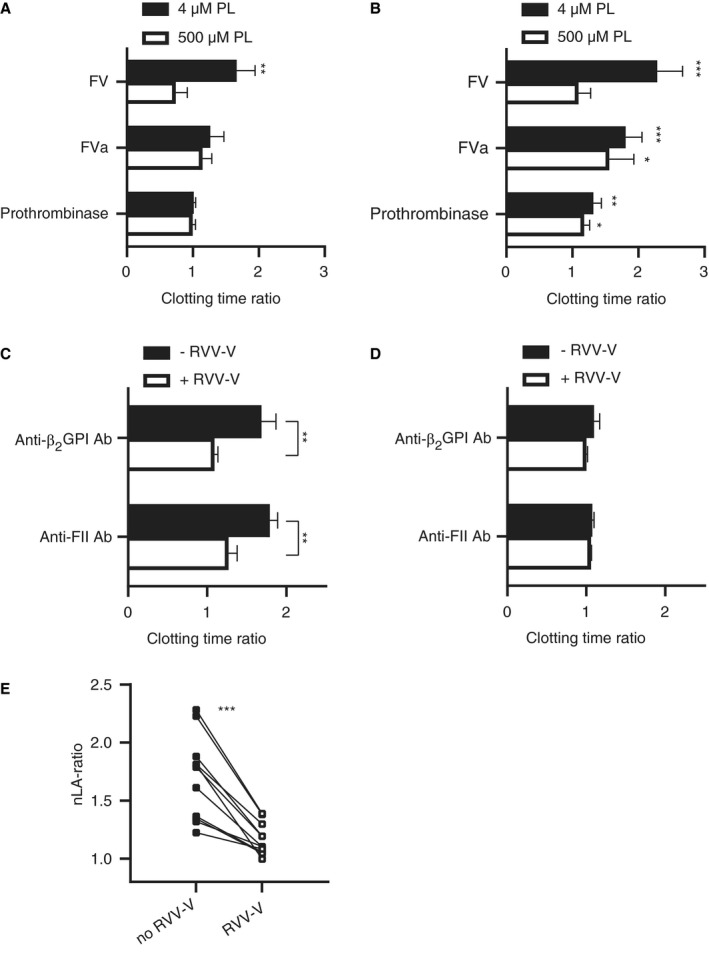
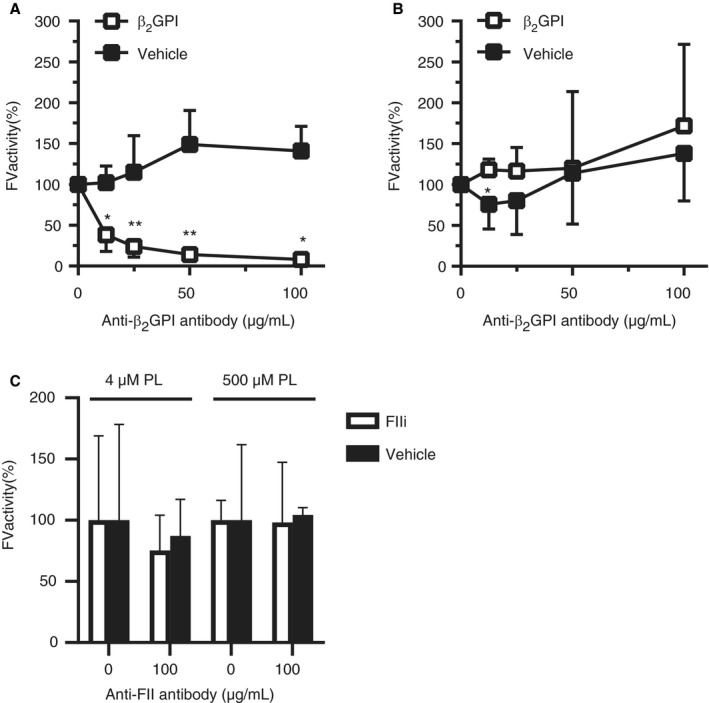
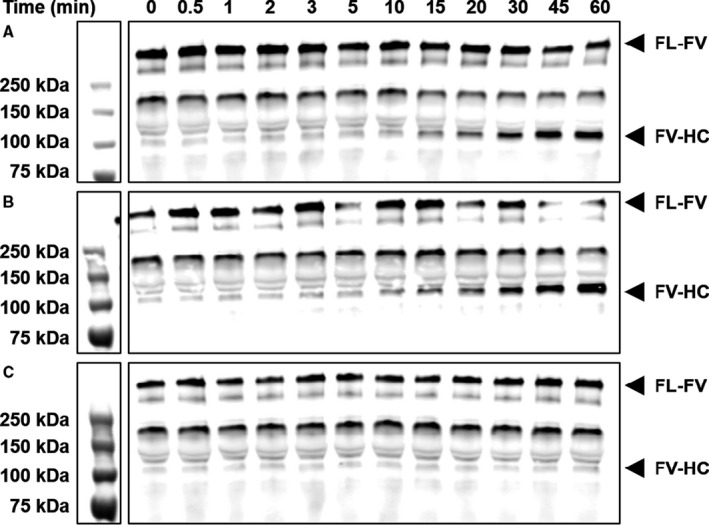
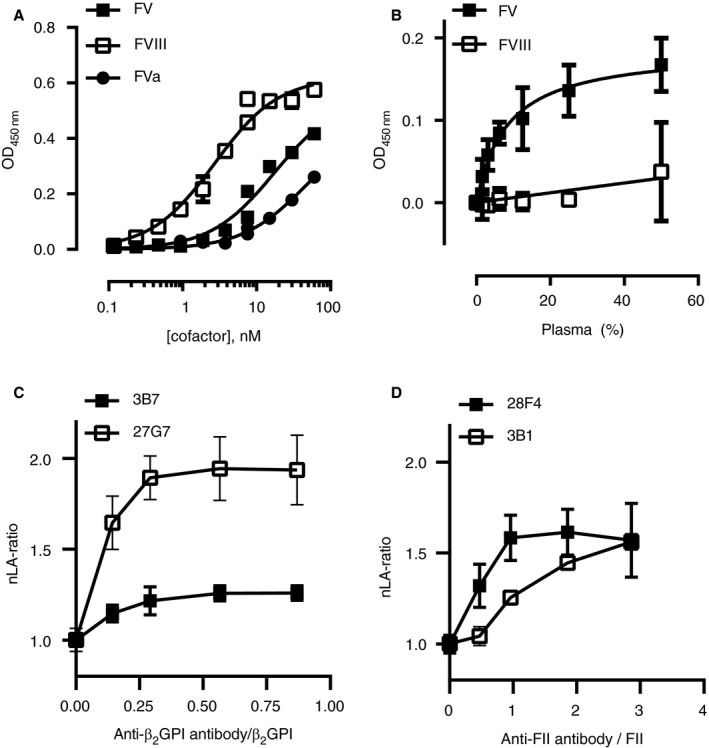
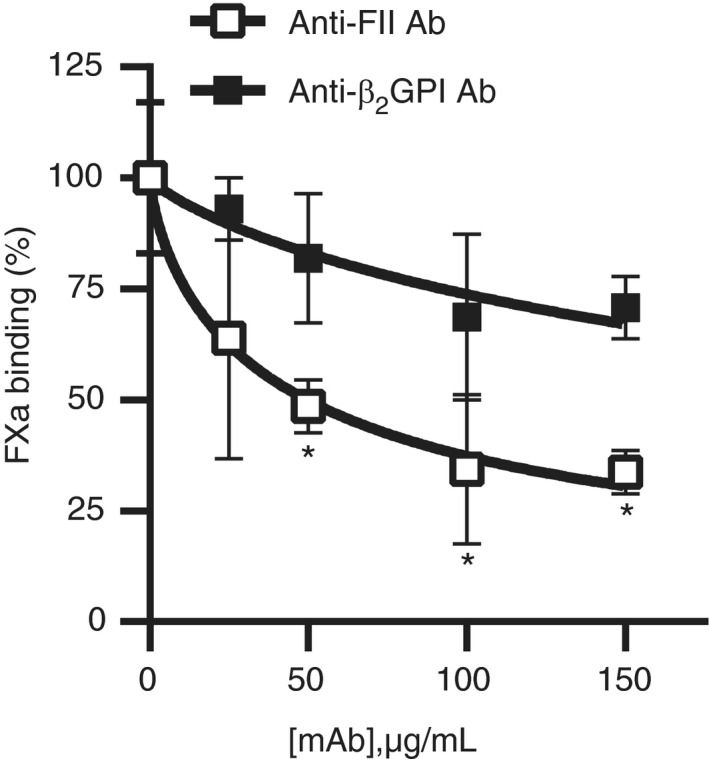
Results: Detection of LA caused by anti-β2GPI or anti-prothrombin antibodies required the presence of the procofactor factor V (FV) in plasma. LA effect disappeared when FV was replaced by activated FV (FVa), both in a model system and in patient plasma, although differences between anti-β2GPI and anti-prothrombin antibodies were observed. Further exploration of the effects of the antibodies on coagulation showed that the anti-β2GPI antibody attenuated FV activation by activated faxtor X (FXa), whereas the anti-prothrombin antibody did not. Binding studies showed that β2GPI--antibody complexes directly interacted with FV with high affinity. Anti-prothrombin complexes caused the LA phenomenon through competition for phospholipid binding sites with coagulation factors as reduced FXa binding to lipospheres was observed with flow cytometry in the presence of these antibodies.
Conclusion: Anti-β2GPI and anti-prothrombin antibodies cause LA through different mechanisms of action: While anti-β2GPI antibodies interfere with FV activation by FXa through a direct interaction with FV, anti-prothrombin antibodies compete with FXa for phospholipid binding sites. These data provide leads for understanding the paradoxical association between thrombosis and a prolonged clotting time in the antiphospholipid syndrome.
Keywords: antiphospholipid antibodies; beta2-glycoprotein I; factor V; lupus anticoagulant; prothrombin.
© 2021 The Authors. Journal of Thrombosis and Haemostasis published by Wiley Periodicals LLC on behalf of International Society on Thrombosis and Haemostasis.
Conflict of interest statement
There are no conflicts of interest reported by any of the authors.
Figures
References
-
- Keeling D, Mackie I, Moore GW, Greer IA, Greaves M. Guidelines on the investigation and management of antiphospholipid syndrome. Br J Haematol. 2012;157(1):47‐58. - PubMed
-
- Limper M, de Leeuw K, Lely AT, et al. Diagnosing and treating antiphospholipid syndrome: A consensus paper. Neth J Med. 2019;77(3):98‐108. - PubMed
-
- Miyakis S, Lockshin MD, Atsumi T, et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J Thromb Haemost. 2006;4(2):295‐306. - PubMed
-
- Pengo V, Banzato A, Denas G, et al. Correct laboratory approach to APS diagnosis and monitoring. Autoimmun Rev. 2013;12(8):832‐834. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
