

The importance of anosmia, ageusia and age in community presentation of symptomatic and asymptomatic SARS-CoV-2 infection in Louisiana, USA; a cross-sectional prevalence study
- PMID: 33421576
- PMCID: PMC7787079
- DOI: 10.1016/j.cmi.2020.12.029
The importance of anosmia, ageusia and age in community presentation of symptomatic and asymptomatic SARS-CoV-2 infection in Louisiana, USA; a cross-sectional prevalence study
Abstract
Objective: While many seroprevalence studies of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) have been performed, few are demographically representative. This investigation focused on defining the nature and frequency of symptomatic and asymptomatic SARS-CoV-2 infection in a representative, cross-sectional sample of communities in Louisiana, USA.
Methods: A sample of 4778 adults from New Orleans and Baton Rouge, Louisiana were given a survey of symptoms and co-morbidities, nasopharyngeal swab to test for active infection (PCR), and blood draw to test for past infection (IgG). Odds ratios, cluster analysis, quantification of virus and antibody, and linear modelling were used to understand whether certain symptoms were associated with a positive test, how symptoms grouped together, whether virus or antibody varied by symptom status, and whether being symptomatic was different across the age span.
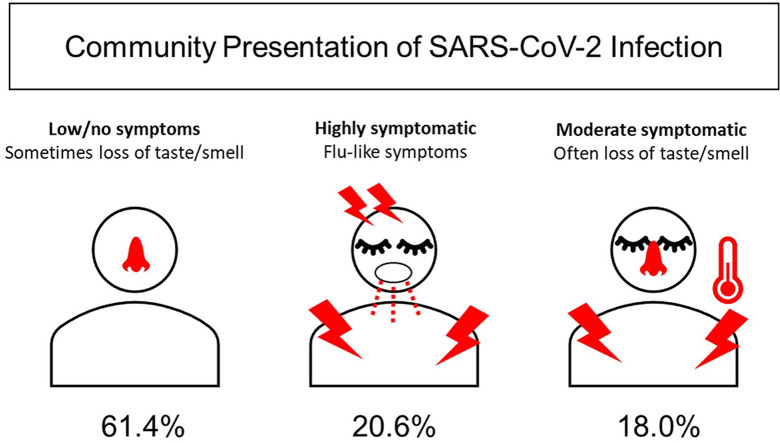
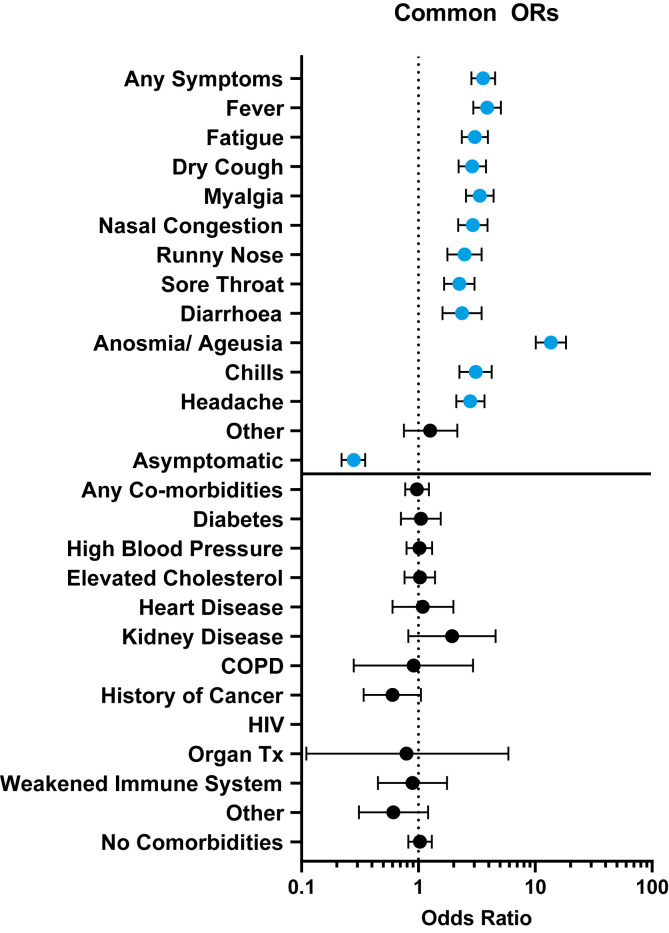
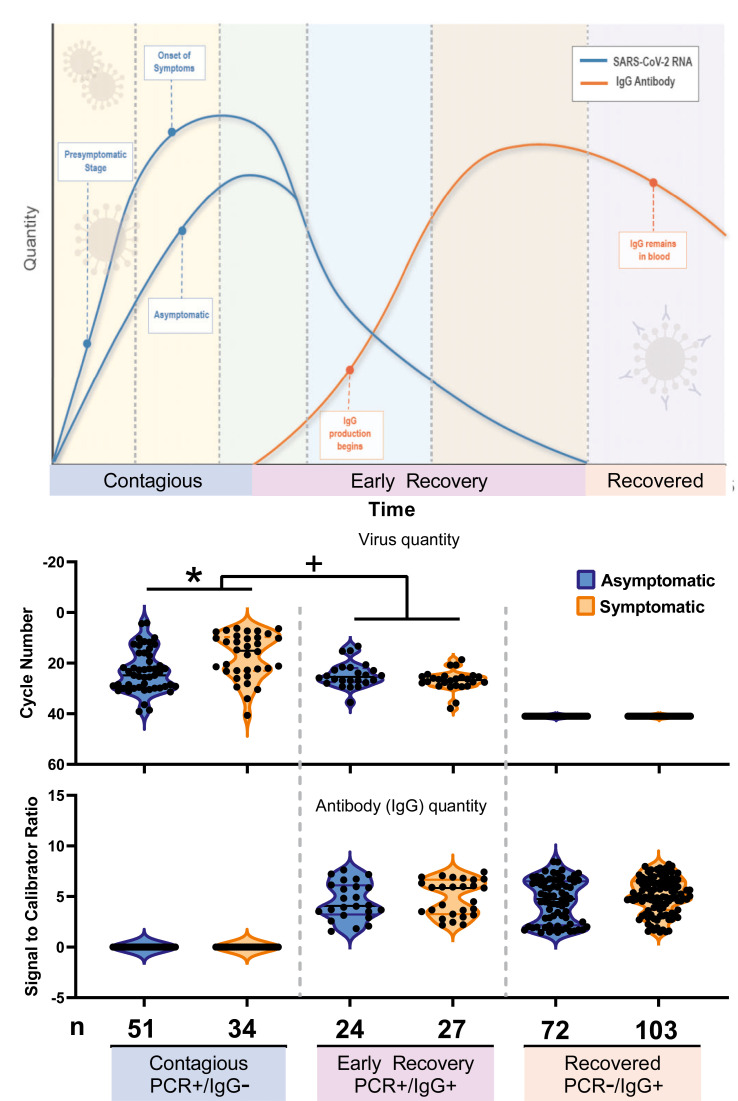
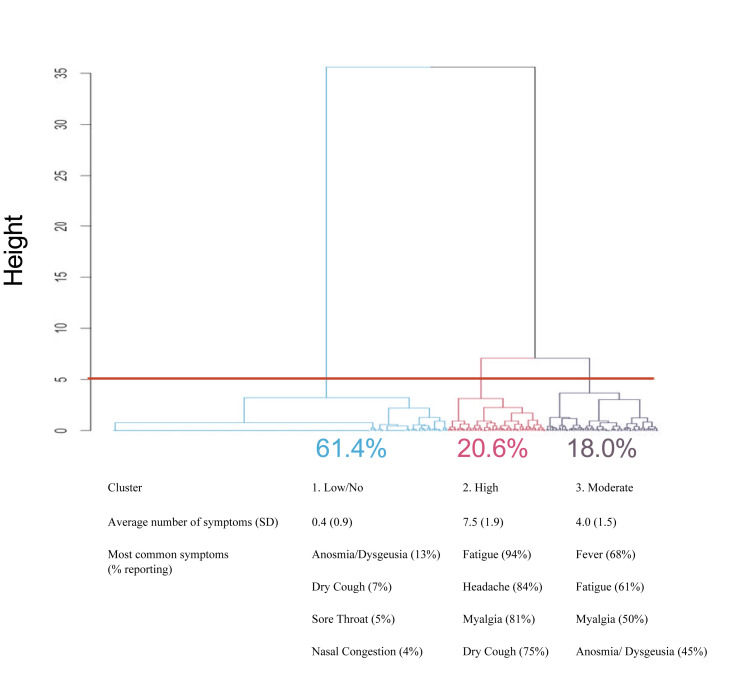
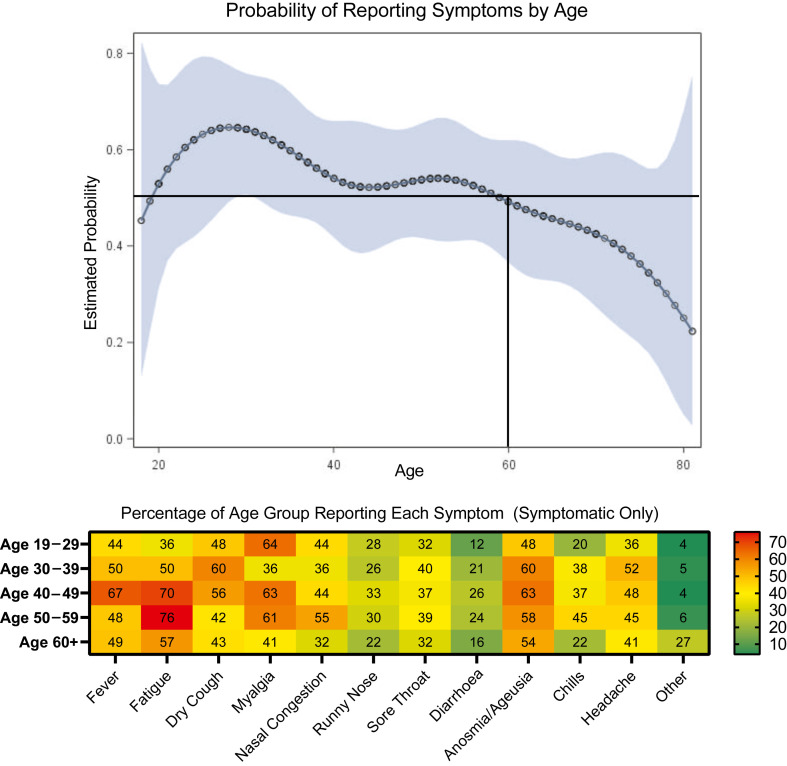
Results: Reported anosmia/ageusia was strongly associated with a positive test; 40.6% (93/229) tested positive versus 4.8% (218/4549) positivity in those who did not report anosmia/ageusia (OR 13.6, 95% CI 10.1-18.3). Of the people who tested positive, 47.3% (147/311) were completely asymptomatic. Symptom presentation clustered into three groups; low/no symptoms (0.4 ± 0.9, mean ± SD), highly symptomatic (7.5 ± 1.9) or moderately symptomatic (4.0 ± 1.5). Quantity of virus was lower in the asymptomatic versus symptomatic group (cycle number 23.3 ± 8.3 versus 17.3 ± 9.0; p < 0.001). Modelling the probability of symptoms showed changes with age; the highest probability of reporting symptoms was 64.6% (95% CI 50.4-76.5) at age 29 years, which decreased to a probability of 49.3% (95% CI 36.6-62.0) at age 60 years and only 25.1% (95% CI 5.0-68.1) at age 80 years.
Conclusion: Anosmia/ageusia can be used to differentiate SARS-CoV-2 infection from other illnesses, and, given the high ratio of asymptomatic individuals, contact tracing should include those without symptoms. Regular testing in congregant settings of those over age 60 years may help mitigate asymptomatic spread.
Keywords: Ageusia; Anosmia; Asymptomatic infection; Severe acute respiratory syndrome coronavirus 2 prevalence; Symptom incidence.
Copyright © 2021 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- Emmenegger M., De Cecco E., Lamparter D., Jacquat R.P.B., Ebner D., Schneider M.M. Early plateau of SARS-CoV-2 seroprevalence identified by tripartite immunoassay in a large population. medRxiv. 2020:2020. 05.31.20118554.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
