LASSO-Based Machine Learning Algorithm for Prediction of Lymph Node Metastasis in T1 Colorectal Cancer
- PMID: 33421980
- PMCID: PMC8291173
- DOI: 10.4143/crt.2020.974
LASSO-Based Machine Learning Algorithm for Prediction of Lymph Node Metastasis in T1 Colorectal Cancer
Abstract
Purpose: The role of tumor-infiltrating lymphocytes (TILs) in predicting lymph node metastasis (LNM) in patients with T1 colorectal cancer (CRC) remains unclear. Furthermore, clinical utility of a machine learning-based approach has not been widely studied.
Materials and methods: Immunohistochemistry for TILs against CD3, CD8, and forkhead box P3 in both center and invasive margin of the tumor were performed using surgically resected T1 CRC slides. Three hundred and sixteen patients were enrolled and categorized into training (n=221) and validation (n=95) sets via random sampling. Using clinicopathologic variables including TILs, the least absolute shrinkage and selection operator (LASSO) regression model was applied for variable selection and predictive signature building in the training set. The predictive accuracy of our model and the Japanese criteria were compared using area under the receiver operating characteristic (AUROC), net reclassification improvement (NRI)/integrated discrimination improvement (IDI), and decision curve analysis (DCA) in the validation set.
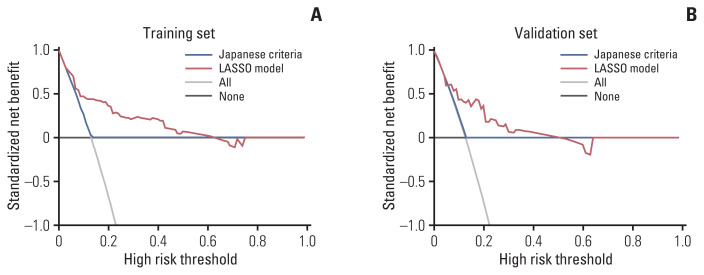
Results: LNM was detected in 29 (13.1%) and 12 (12.6%) patients in training and validation sets, respectively. Nine variables were selected and used to generate the LASSO model. Its performance was similar in training and validation sets (AUROC, 0.795 vs. 0.765; p=0.747). In the validation set, the LASSO model showed better outcomes in predicting LNM than Japanese criteria, as measured by AUROC (0.765 vs. 0.518, p=0.003) and NRI (0.447, p=0.039)/IDI (0.121, p=0.034). DCA showed positive net benefits in using our model.
Conclusion: Our LASSO model incorporating histopathologic parameters and TILs showed superior performance compared to conventional Japanese criteria in predicting LNM in patients with T1 CRC.
Keywords: LASSO; Lymph node; Machine learning; T1 colorectal cancer; Tumor-infiltrating lymphocytes.
Conflict of interest statement
Conflict of interest relevant to this article was not reported.
Figures


References
-
- Kitajima K, Fujimori T, Fujii S, Takeda J, Ohkura Y, Kawamata H, et al. Correlations between lymph node metastasis and depth of submucosal invasion in submucosal invasive colorectal carcinoma: a Japanese collaborative study. J Gastroenterol. 2004;39:534–43. - PubMed
-
- Kobayashi H, Mochizuki H, Morita T, Kotake K, Teramoto T, Kameoka S, et al. Characteristics of recurrence after curative resection for T1 colorectal cancer: Japanese multicenter study. J Gastroenterol. 2011;46:203–11. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials