

Machine learning-based prediction models for accidental hypothermia patients
- PMID: 33422146
- PMCID: PMC7797142
- DOI: 10.1186/s40560-021-00525-z
Machine learning-based prediction models for accidental hypothermia patients
Abstract
Background: Accidental hypothermia is a critical condition with high risks of fatal arrhythmia, multiple organ failure, and mortality; however, there is no established model to predict the mortality. The present study aimed to develop and validate machine learning-based models for predicting in-hospital mortality using easily available data at hospital admission among the patients with accidental hypothermia.
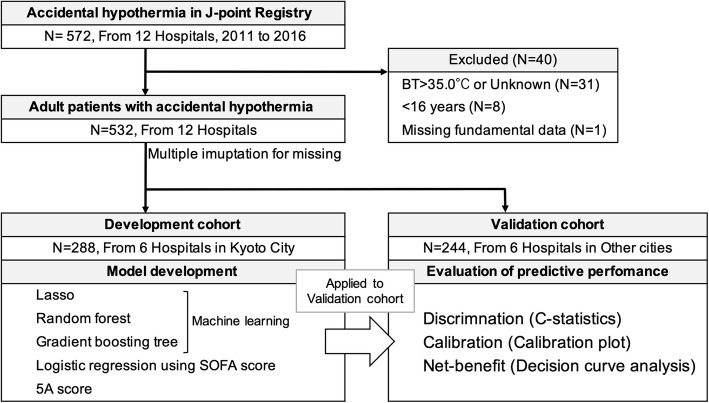
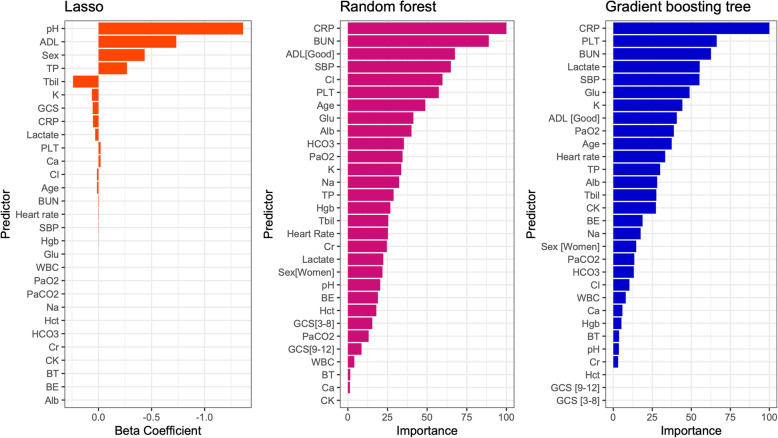
Method: This study was secondary analysis of multi-center retrospective cohort study (J-point registry) including patients with accidental hypothermia. Adult patients with body temperature 35.0 °C or less at emergency department were included. Prediction models for in-hospital mortality using machine learning (lasso, random forest, and gradient boosting tree) were made in development cohort from six hospitals, and the predictive performance were assessed in validation cohort from other six hospitals. As a reference, we compared the SOFA score and 5A score.
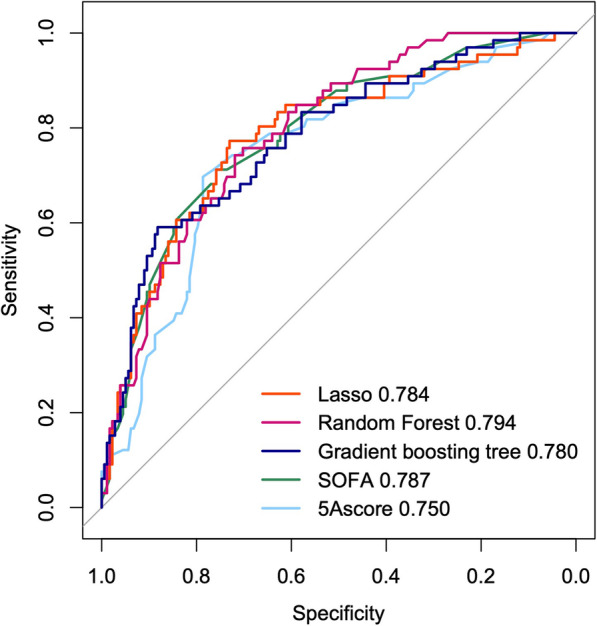
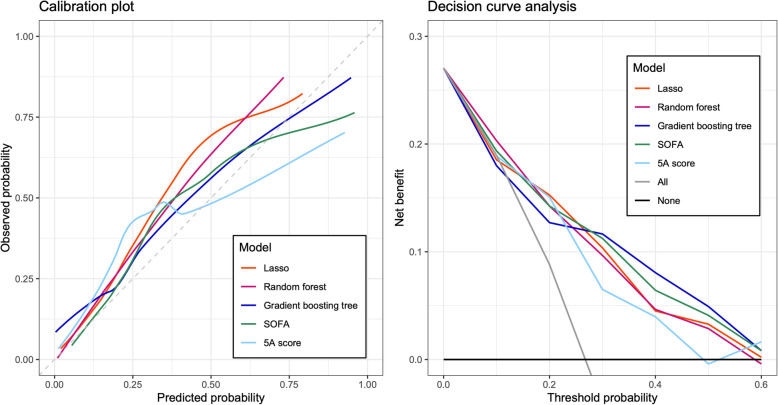
Results: We included total 532 patients in the development cohort [N = 288, six hospitals, in-hospital mortality: 22.0% (64/288)], and the validation cohort [N = 244, six hospitals, in-hospital mortality 27.0% (66/244)]. The C-statistics [95% CI] of the models in validation cohorts were as follows: lasso 0.784 [0.717-0.851] , random forest 0.794[0.735-0.853], gradient boosting tree 0.780 [0.714-0.847], SOFA 0.787 [0.722-0.851], and 5A score 0.750[0.681-0.820]. The calibration plot showed that these models were well calibrated to observed in-hospital mortality. Decision curve analysis indicated that these models obtained clinical net-benefit.
Conclusion: This multi-center retrospective cohort study indicated that machine learning-based prediction models could accurately predict in-hospital mortality in validation cohort among the accidental hypothermia patients. These models might be able to support physicians and patient's decision-making. However, the applicability to clinical settings, and the actual clinical utility is still unclear; thus, further prospective study is warranted to evaluate the clinical usefulness.
Keywords: Accidental hypothermia; Artificial intelligence; Gradient boosting tree; Lasso; Machine learning; Prediction; Random forest.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Matsuyama T, Morita S, Ehara N, Miyamae N, Okada Y, Jo T, Sumida Y, Okada N, Watanabe M, Nozawa M, Tsuruoka A, Fujimoto Y, Okumura Y, Kitamura T, Ohta B. Characteristics and outcomes of accidental hypothermia in Japan: the J-Point registry. Emerg Med J. 2018;35(11):659–66. 10.1136/emermed-2017-207238. Epub 2018 Jun 9. PMID: 29886414. - PubMed
-
- Medicine JAfA: The clinical characteristics of hypothermic patients in the winter of Japan—the final report of Hypothermia STUDY 2011. J Jpn Assoc Acute Med. 2013;24:12.
-
- Okada Y, Matsuyama T, Morita S, Ehara N, Miyamae N, Jo T, Sumida Y, Okada N, Watanabe M, Nozawa M, et al. The development and validation of a "5A" severity scale for predicting in-hospital mortality after accidental hypothermia from J-point registry data. J Intensive Care. 2019;7:27. doi: 10.1186/s40560-019-0384-2. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
