

A neural network to predict the knee adduction moment in patients with osteoarthritis using anatomical landmarks obtainable from 2D video analysis
- PMID: 33422707
- PMCID: PMC7925428
- DOI: 10.1016/j.joca.2020.12.017
A neural network to predict the knee adduction moment in patients with osteoarthritis using anatomical landmarks obtainable from 2D video analysis
Abstract
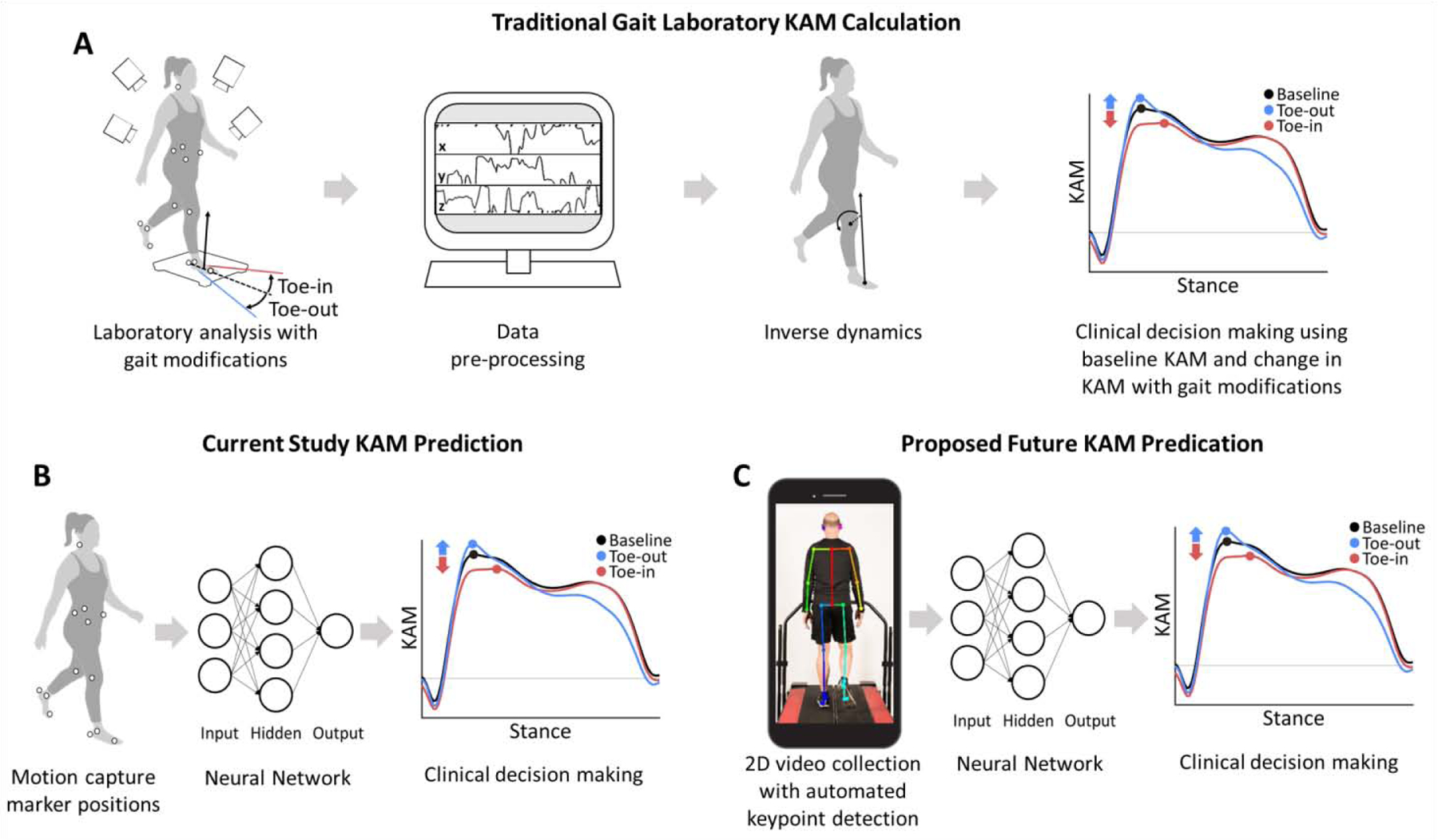
Objective: The knee adduction moment (KAM) can inform treatment of medial knee osteoarthritis; however, measuring the KAM requires an expensive gait analysis laboratory. We evaluated the feasibility of predicting the peak KAM during natural and modified walking patterns using the positions of anatomical landmarks that could be identified from video analysis.
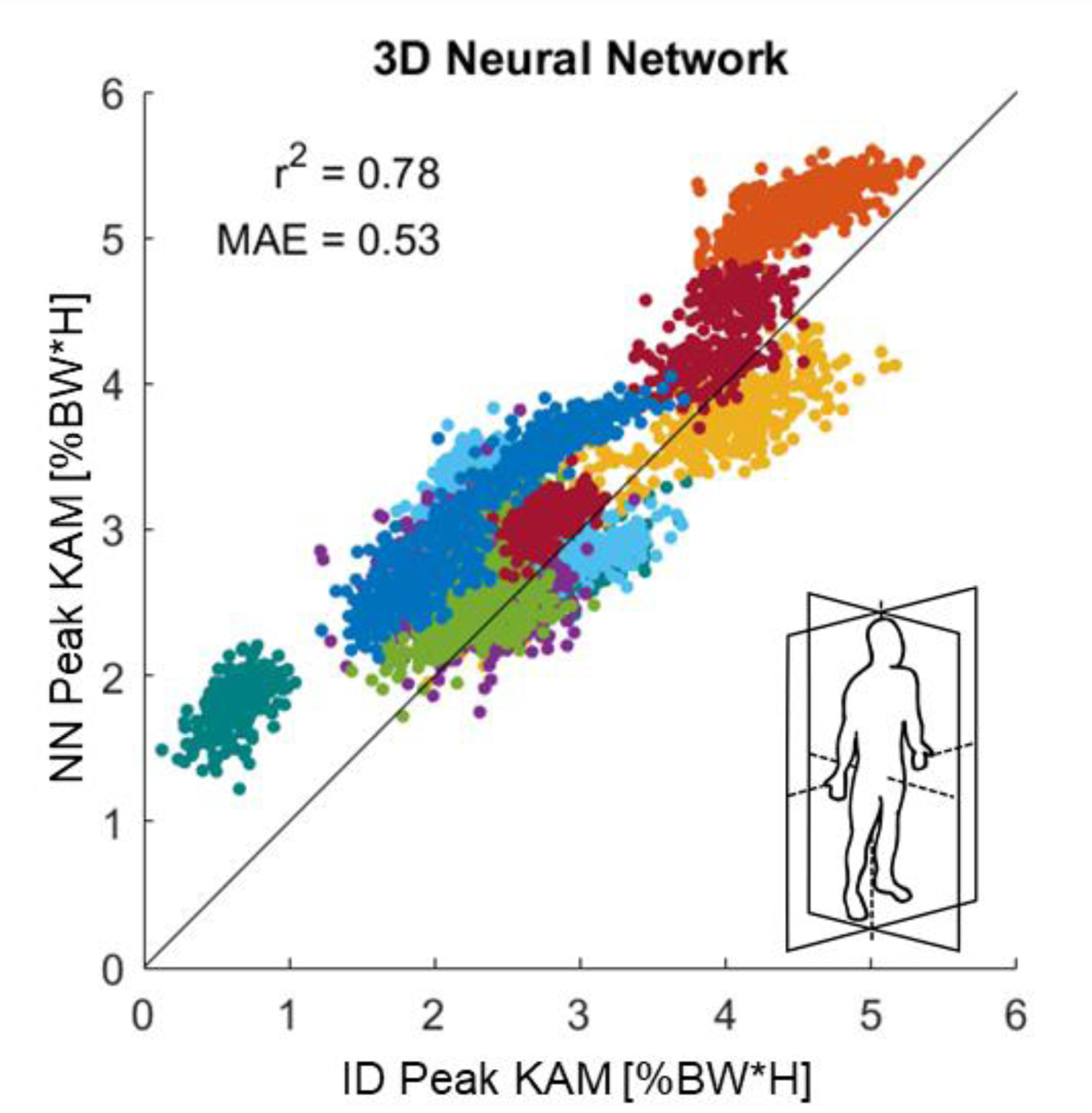
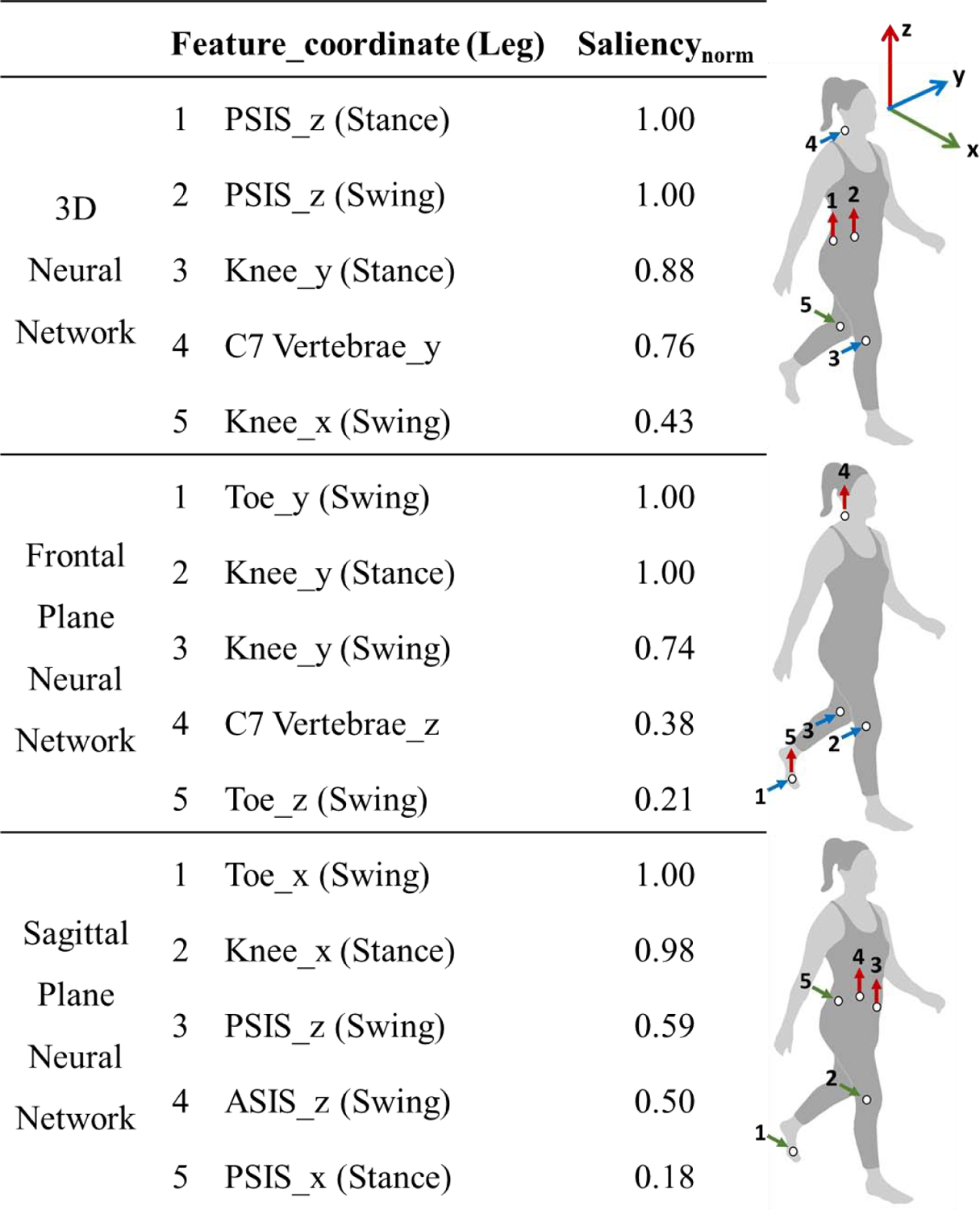
Method: Using inverse dynamics, we calculated the KAM for 86 individuals (64 with knee osteoarthritis, 22 without) walking naturally and with foot progression angle modifications. We trained a neural network to predict the peak KAM using the 3-dimensional positions of 13 anatomical landmarks measured with motion capture (3D neural network). We also trained models to predict the peak KAM using 2-dimensional subsets of the dataset to simulate 2-dimensional video analysis (frontal and sagittal plane neural networks). Model performance was evaluated on a held-out, 8-person test set that included steps from all trials.
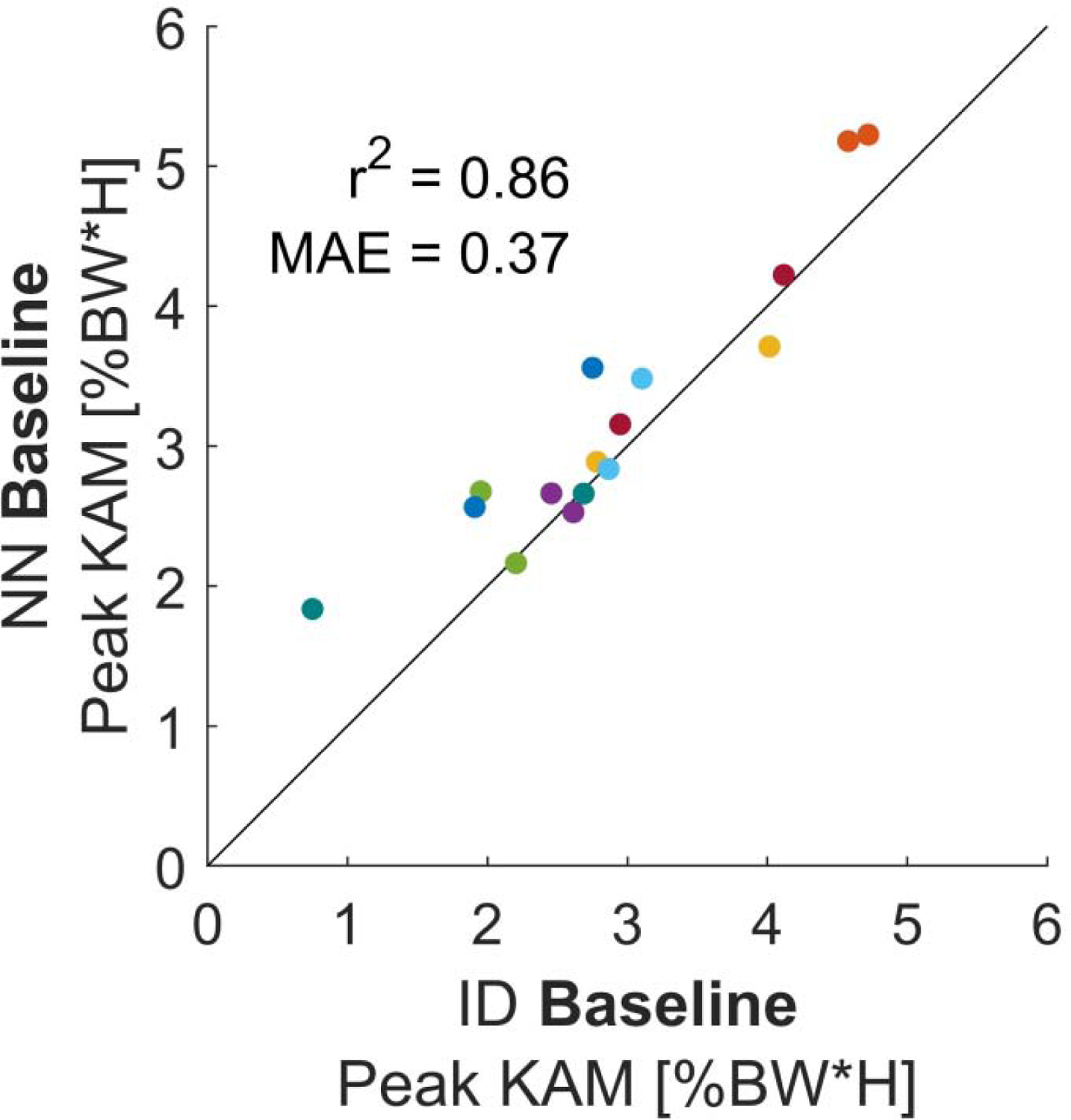
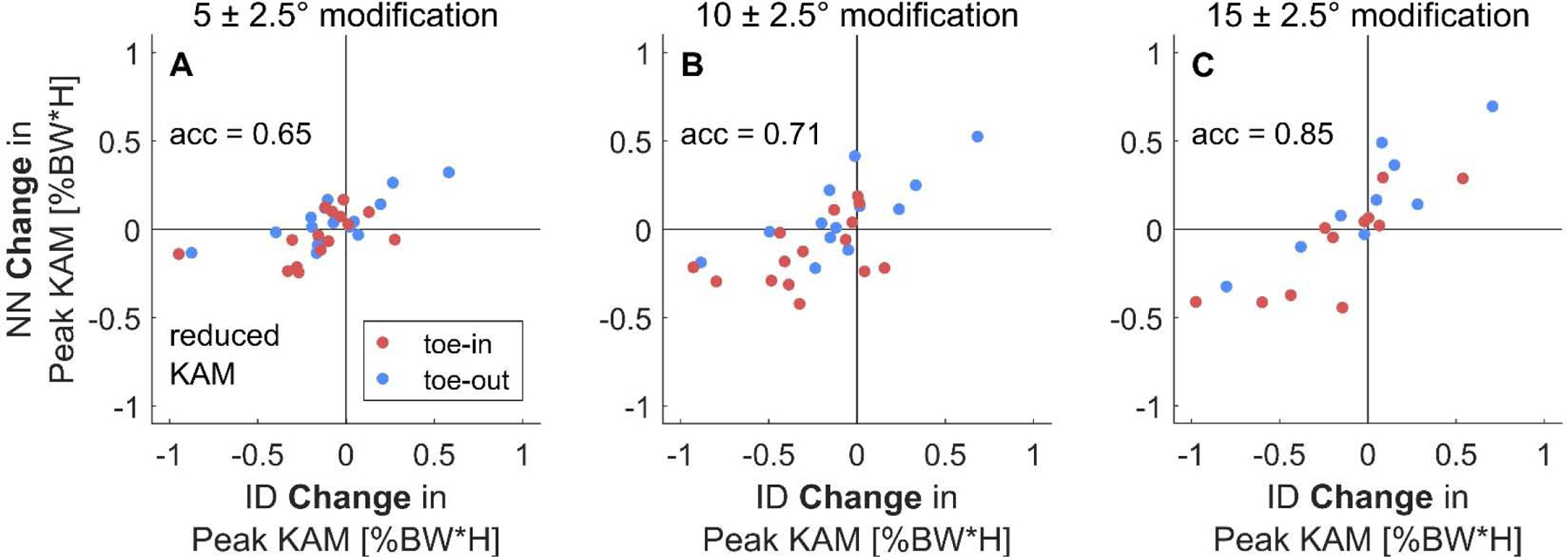
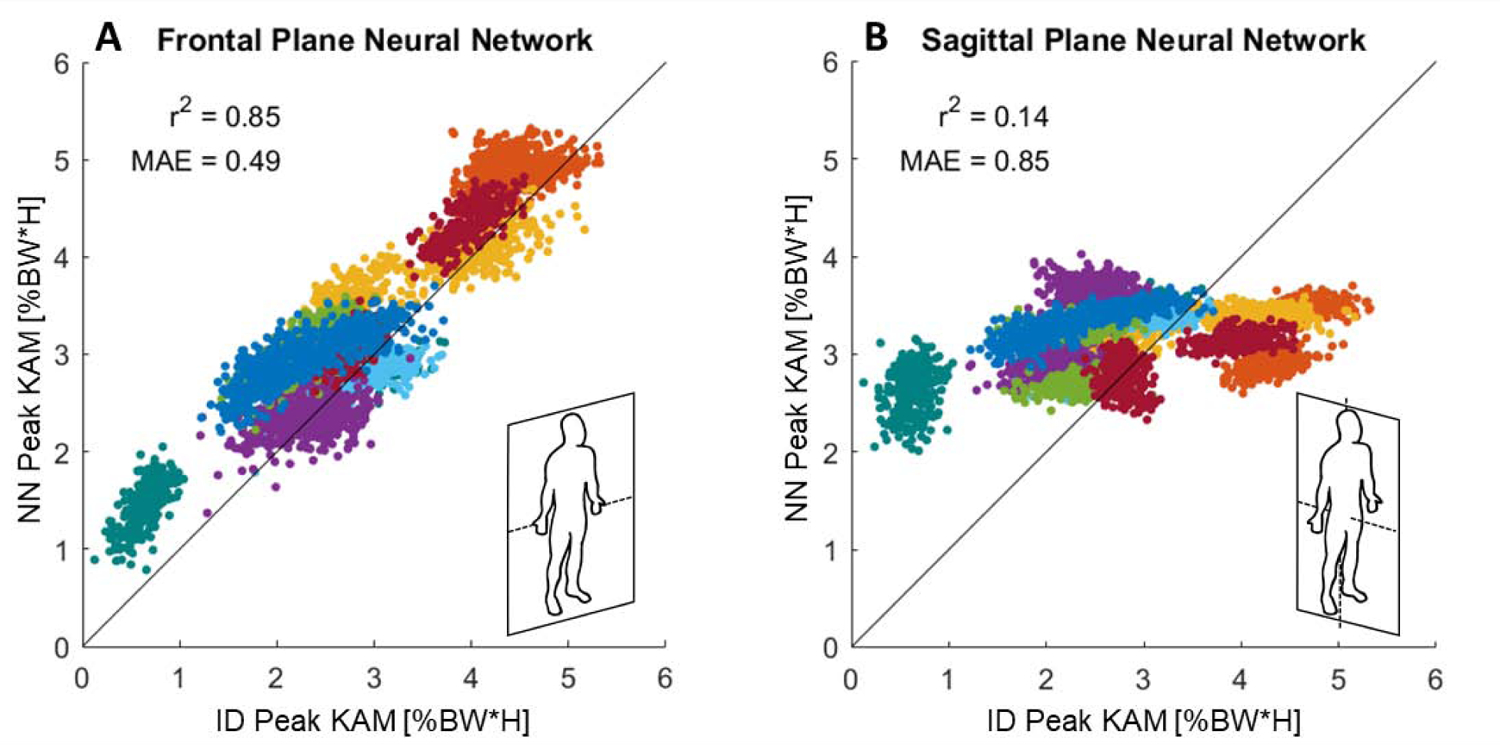
Results: The 3D neural network predicted the peak KAM for all test steps with r2( Murray et al., 2012) 2 = 0.78. This model predicted individuals' average peak KAM during natural walking with r2( Murray et al., 2012) 2 = 0.86 and classified which 15° foot progression angle modifications reduced the peak KAM with accuracy = 0.85. The frontal plane neural network predicted peak KAM with similar accuracy (r2( Murray et al., 2012) 2 = 0.85) to the 3D neural network, but the sagittal plane neural network did not (r2( Murray et al., 2012) 2 = 0.14).
Conclusion: Using the positions of anatomical landmarks from motion capture, a neural network accurately predicted the peak KAM during natural and modified walking. This study demonstrates the feasibility of measuring the peak KAM using positions obtainable from 2D video analysis.
Keywords: Gait; Knee adduction moment; Machine learning; Neural network; Osteoarthritis; Video motion analysis.
Copyright © 2021 Osteoarthritis Research Society International. All rights reserved.
Conflict of interest statement
Competing Interests
The authors have no conflicts of interest to declare.
Figures
References
-
- Murray CJL, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2197–2223. doi: 10.1016/S0140-6736(12)61689-4 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
