

Infectious titres of human papillomaviruses (HPVs) in patient lesions, methodological considerations in evaluating HPV infectivity and implications for the efficacy of high-level disinfectants
- PMID: 33422988
- PMCID: PMC7808919
- DOI: 10.1016/j.ebiom.2020.103165
Infectious titres of human papillomaviruses (HPVs) in patient lesions, methodological considerations in evaluating HPV infectivity and implications for the efficacy of high-level disinfectants
Abstract
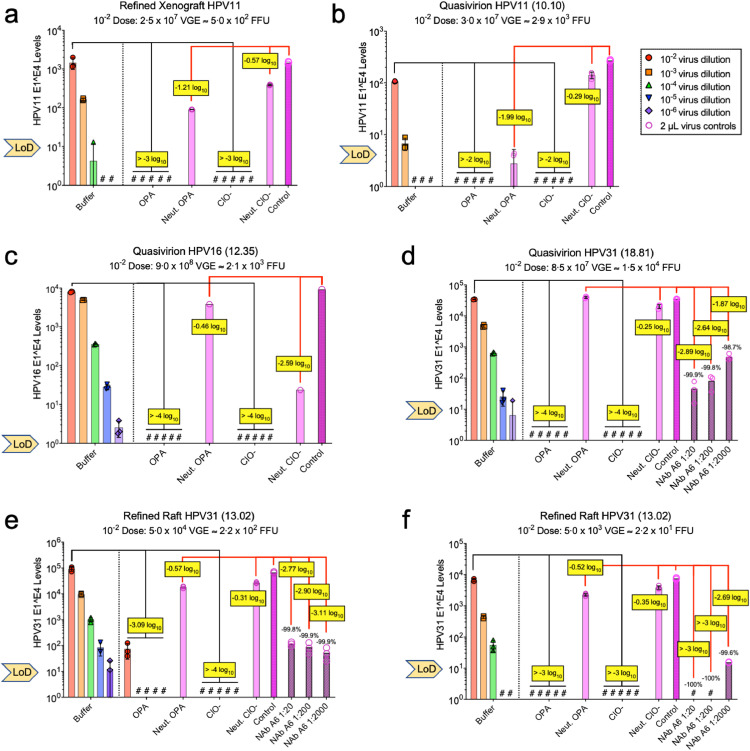
Background: Recent publications from a single research group have suggested that aldehyde-based high-level disinfectants (HLDs), such as ortho-phthalaldehyde (OPA), are not effective at inactivating HPVs and that therefore, patients may be at risk of HPV infection from medical devices. These results could have significant public health consequences and therefore necessitated evaluation of their reproducibility and clinical relevance.
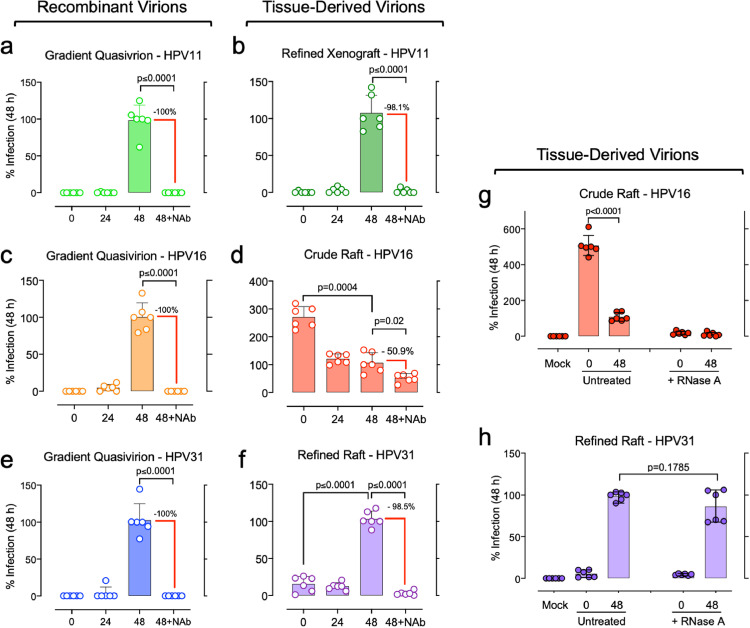
Methods: We developed methods and used standardised controls to: (1) quantify the infectious levels of clinically-sourced HPVs from patient lesions and compare them to laboratory-derived HPVs, (2) evaluate experimental factors that should be controlled to ensure consistent and reproducible infectivity measurements of different HPV genotypes, and (3) determine the efficacy of select HLDs.
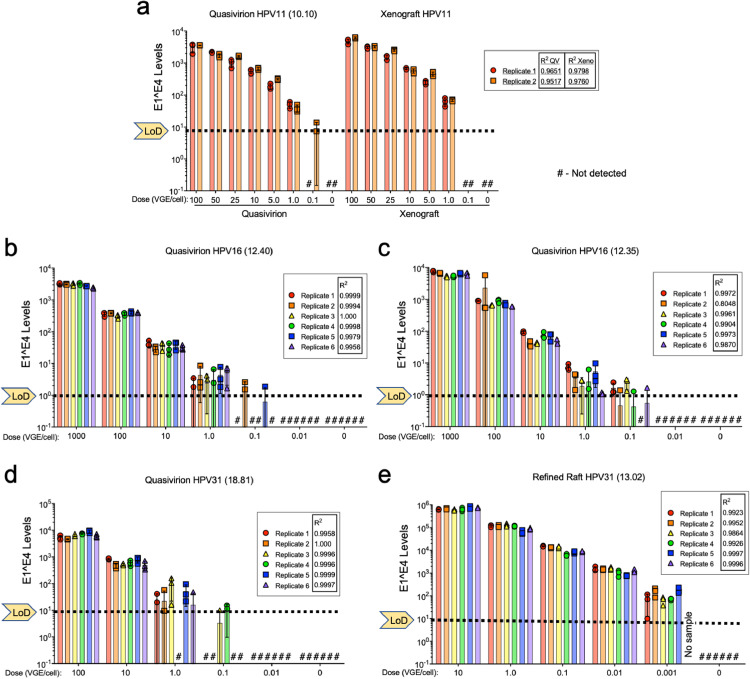
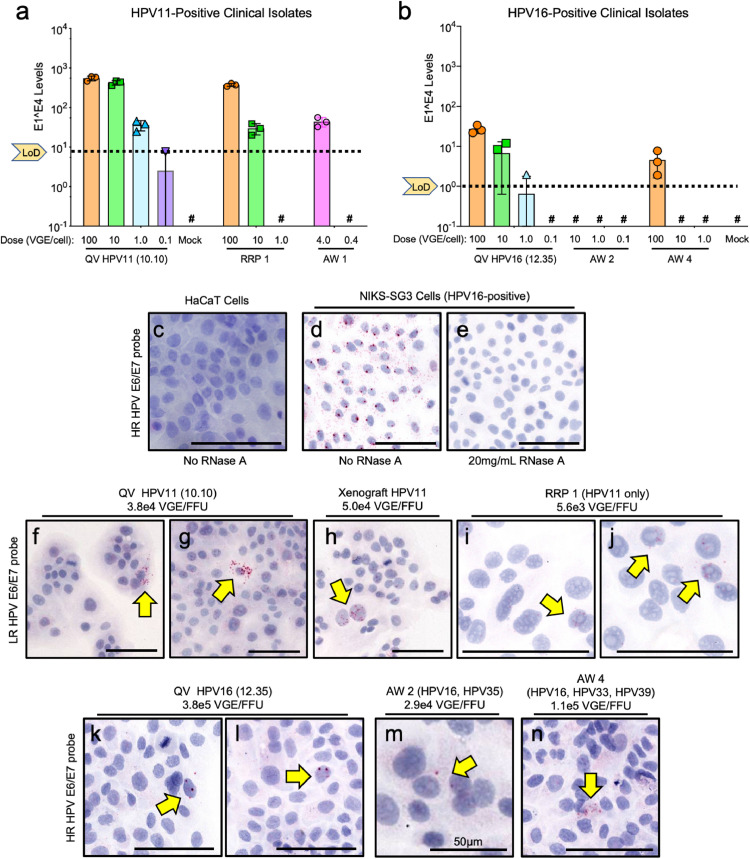
Findings: A novel focus forming unit (FFU) infectivity assay demonstrated that exfoliates from patient anogenital lesions and respiratory papillomas yielded infectious HPV burdens up to 2.7 × 103 FFU; therefore, using 2.2 × 102 to 1.0 × 104 FFU of laboratory-derived HPVs in disinfection assays provides a relevant range for clinical exposures. RNase and neutralising antibody sensitivities were used to ensure valid infectivity measures of tissue-derived and recombinant HPV preparations. HPV infectivity was demonstrated over a dynamic range of 4-5 log10; and disinfection with OPA and hypochlorite was achieved over 3 to >4 log10 with multiple genotypes of tissue-derived and recombinant HPV isolates.
Interpretation: This work, along with a companion publication from an independent lab in this issue, address a major public health question by showing that HPVs are susceptible to HLDs.
Funding: Advanced Sterilization Products; US NIH (R01CA207368, U19AI084081, P30CA118100).
Keywords: High-level disinfectant; Medical devices; Nosocomial infection; Oncogenic virus; Sexually transmitted disease; Virus disinfection.
Copyright © 2020 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest M.A.O. reports grants, personal fees, and non-financial support from Advanced Sterilization Products, grants from U.S. National Institutes of Health, during the conduct of the study; A.G.W. reports personal fees and non-financial support from ASCCP, non-financial support from ACOG, non-financial support from Loktal Medical Electronics, personal fees and non-financial support from CSCCP (Chinese Society for colposcopy and cervical pathology, personal fees and non-financial support from Henan People's Regional Hospital, personal fees from Southcentral Foundation (Alaska Native Corp), non-financial support from FECOLSOG (Colombian colposcopy society), non-financial support from COMEGIC (Mexican colposcopy society), non-financial support from Doctors Hospital at Renaissance, non-financial support from MD Anderson, non-financial support from Univ Texas Rio Grande Valley, non-financial support from Global Coalition against Cervical Cancer, non-financial support from AIDS Malignancy Consortium, personal fees and non-financial support from Deaconess Beth Israel Hospital, personal fees and non-financial support from Texas Tech University, personal fees and non-financial support from ABPTGIC (Brazilian colposcopy society), outside the submitted work. V.B., N.A.P, R.T.S., E.C.B. and R.M. have nothing to disclose. A.S., J.Y. and M.R. are employees of Advanced Sterilization Products. G.E. is an employee and shareholder of Johnson & Johnson, which was the parent company for Advanced Sterilization Products and Janssen Pharmaceutica NV at the time the research was conducted.
Figures

Similar articles
-
Dynamics of papillomavirus in vivo disease formation & susceptibility to high-level disinfection-Implications for transmission in clinical settings.EBioMedicine. 2021 Jan;63:103177. doi: 10.1016/j.ebiom.2020.103177. Epub 2021 Jan 6. EBioMedicine. 2021. PMID: 33421945 Free PMC article.
-
Inactivation of Polyomavirus SV40 as Surrogate for Human Papillomaviruses by Chemical Disinfectants.Viruses. 2021 Nov 2;13(11):2207. doi: 10.3390/v13112207. Viruses. 2021. PMID: 34835013 Free PMC article.
-
Susceptibility of HPV16 and 18 to high level disinfectants indicated for semi-critical ultrasound probes.J Med Virol. 2016 Jun;88(6):1076-80. doi: 10.1002/jmv.24421. Epub 2015 Nov 13. J Med Virol. 2016. PMID: 26519866 Free PMC article.
-
Biology and pathological associations of the human papillomaviruses: a review.Malays J Pathol. 1998 Jun;20(1):1-10. Malays J Pathol. 1998. PMID: 10879257 Review.
-
Human papillomavirus infections: warts or cancer?Cold Spring Harb Perspect Biol. 2013 Jul 1;5(7):a012997. doi: 10.1101/cshperspect.a012997. Cold Spring Harb Perspect Biol. 2013. PMID: 23685995 Free PMC article. Review.
Cited by
-
Protamine Sulfate Is a Potent Inhibitor of Human Papillomavirus Infection In Vitro and In Vivo.Antimicrob Agents Chemother. 2022 Jan 18;66(1):e0151321. doi: 10.1128/AAC.01513-21. Epub 2021 Nov 1. Antimicrob Agents Chemother. 2022. PMID: 34723633 Free PMC article.
-
A Novel In Vivo Model of Laryngeal Papillomavirus-Associated Disease Using Mus musculus Papillomavirus.Viruses. 2022 May 8;14(5):1000. doi: 10.3390/v14051000. Viruses. 2022. PMID: 35632742 Free PMC article.
-
Electrochemical Resistive DNA Biosensor for the Detection of HPV Type 16.Molecules. 2021 Jun 5;26(11):3436. doi: 10.3390/molecules26113436. Molecules. 2021. PMID: 34198893 Free PMC article.
-
New approaches for infective HPV detection, quantification and inactivation: Preventing accidental virus transmission in medical settings.EBioMedicine. 2021 Feb;64:103222. doi: 10.1016/j.ebiom.2021.103222. Epub 2021 Jan 29. EBioMedicine. 2021. PMID: 33524875 Free PMC article. No abstract available.
-
Assessing the reduction of viral infectivity in HPV16/18-positive women after one, two, and three doses of Gardasil-9 (RIFT): Study protocol.PLoS One. 2024 May 20;19(5):e0304080. doi: 10.1371/journal.pone.0304080. eCollection 2024. PLoS One. 2024. PMID: 38768231 Free PMC article.
References
-
- Serrano B, Brotons M, Bosch FX, Bruni L. Epidemiology and burden of HPV-related disease. Best Pract Res Clin Obstet Gynaecol. 2018;47:14–26. - PubMed
-
- Doorbar J. Host control of human papillomavirus infection and disease. Best Pract Res Clin Obstetr Gynaecol. 2018;47:27–41. - PubMed
-
- Ma STC, Yeung AC, Chan PKS, Graham CA. Transvaginal ultrasound probe contamination by the human papillomavirus in the emergency department. Emerg Med J. 2013;30:472–475. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
