

doi: 10.1161/HYPERTENSIONAHA.120.16113.
Epub 2021 Jan 11.
Supine Parasympathetic Withdrawal and Upright Sympathetic Activation Underly Abnormalities of the Baroreflex in Postural Tachycardia Syndrome: Effects of Pyridostigmine and Digoxin
Affiliations
- PMID: 33423527
- PMCID: PMC7946724
- DOI: 10.1161/HYPERTENSIONAHA.120.16113
Item in Clipboard
Supine Parasympathetic Withdrawal and Upright Sympathetic Activation Underly Abnormalities of the Baroreflex in Postural Tachycardia Syndrome: Effects of Pyridostigmine and Digoxin
Hypertension.
2021 Apr.
Abstract
[Figure: see text].
Keywords: baroreflex; digoxin; modified oxford method; orthostasis; postural tachycardia syndrome; pyridostigmine.
Figures
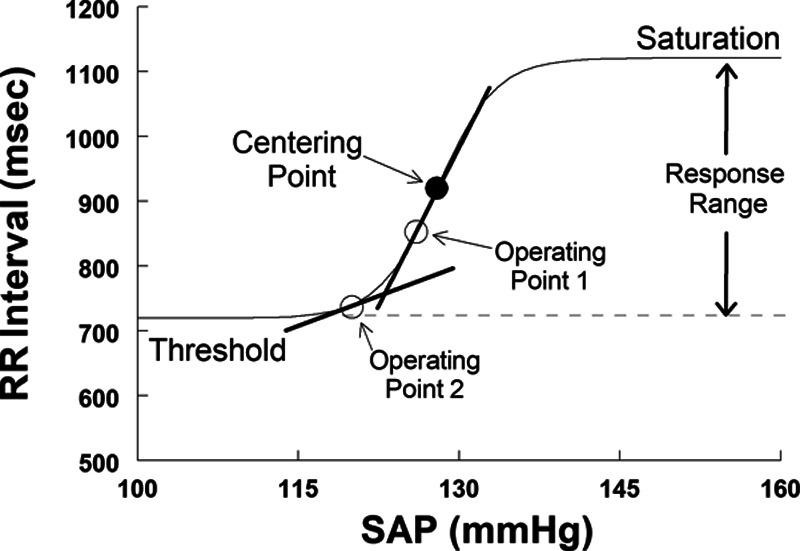
It shows an idealized cardiovagal baroreflex as a sigmoidal relationship between systolic arterial pressure (SAP) and RR interval over a wide range of pressures. The sigmoid curve can be uniquely specified by 4 parameters: the systolic blood pressure (BP; SAP) at the centering point, the slope at the centering point (maximum gain or baroreflex sensitivity, Gmax), the curve’s threshold, and its response range. Operating points define the current state of the system; local slopes at operating points and correspond to the variation of RR interval with variation of BP (BPV) near 0.1 Hz near that particular operating point.
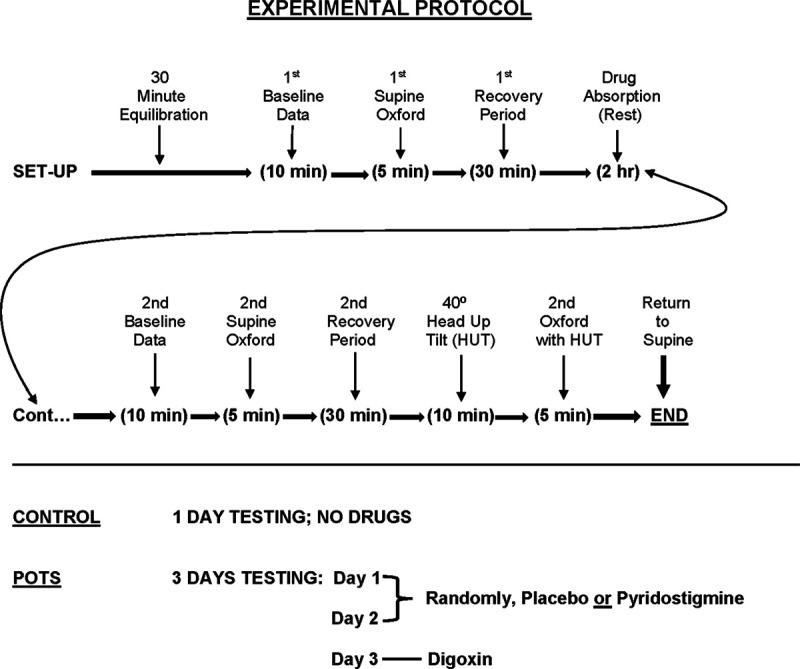
It shows the flow sheet and design of the described studies. The experimental protocol is shown on top and the administration of drugs is shown on the bottom.
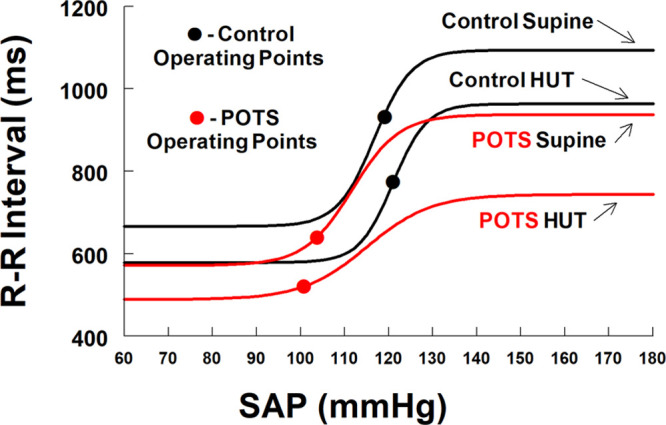
It compares untreated patients with postural tachycardia syndrome (POTS; red lines) with control (black lines) supine and during head-up tilt (HUT). Operating points are shown by red and black circles. Gmax and the response range remained unchanged with tilt in control but were reduced in POTS, and further reduced in POTS when tilted. Additional key features of POTS include left lateral and downwards shifts of centering points and operating points and decreased response range with tilt.
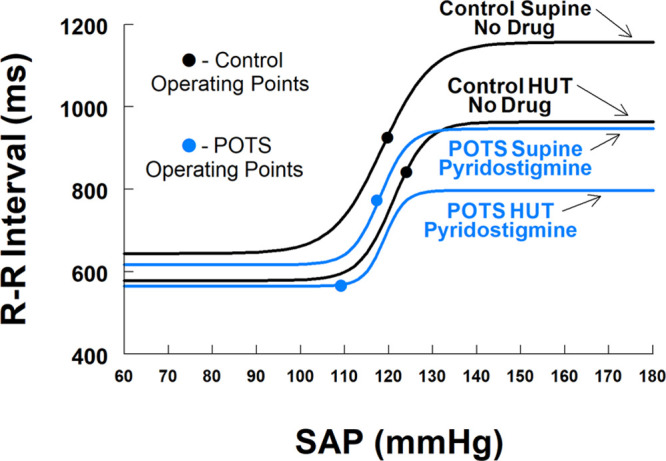
It compares patients with postural tachycardia syndrome (POTS) treated with pyridostigmine (blue lines) with control (black lines) supine and during head-up tilt (HUT). Operating points are shown by blue and black circles. Gmax is restored to near control values supine and upright. Supine systolic arterial pressure (SAP) at centering and operating points are similar to control, but threshold is displaced downwards and response range is curtailed. During tilt centering point, SAP and Gmax were sustained but response range was greatly reduced during tilt contributing to the left shift of the operating point.
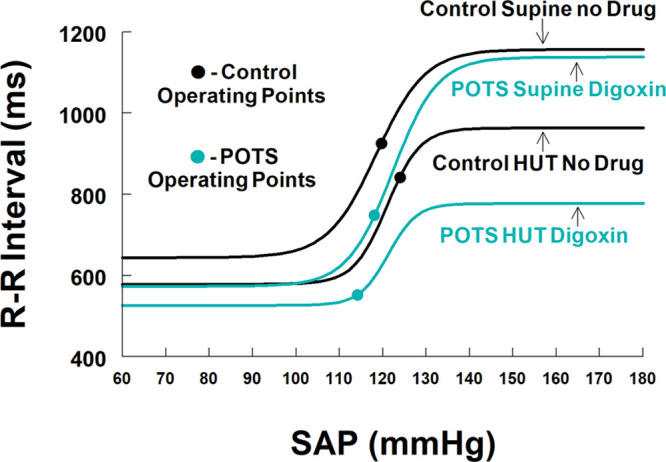
It compares patients with postural tachycardia syndrome (POTS) treated with digoxin (teal lines) with control (black lines) supine and during head-up tilt (HUT). Operating points are shown by cyan and black circles. Digoxin returns the centering point and Gmax of patients with POTS to similar to control values. The response range supine postdigoxin is greater in treated POTS than control. After tilt, threshold was more in POTS while systolic arterial pressure (SAP) at centering point and Gmax were sustained. However, response range decreased markedly with tilt in POTS and contributed to the left shift of the operating point for digoxin and consequently reduced operating point slope.
Comment in
-
Run Vagus Run: Cardiovagal Baroreflex Function and the Postural Tachycardia Syndrome.Hypertension. 2021 Apr;77(4):1245-1247. doi: 10.1161/HYPERTENSIONAHA.121.16578. Epub 2021 Mar 10. Hypertension. 2021. PMID: 33689465 No abstract available.
References
-
- Robertson D. The epidemic of orthostatic tachycardia and orthostatic intolerance. Am J Med Sci. 1999; 317:75–77. doi: 10.1097/00000441-199902000-00001 - PubMed
-
- Stewart JM, Medow MS, DelPozzi A, Messer ZR, Terilli C, Schwartz CE. Middle cerebral O2 delivery during the modified Oxford maneuver increases with sodium nitroprusside and decreases during phenylephrine. Am J Physiol Heart Circ Physiol. 2013; 304:H1576–H1583. doi: 10.1152/ajpheart.00114.2013 - PMC - PubMed
-
- Schondorf R, Low PA. Idiopathic postural orthostatic tachycardia syndrome: an attenuated form of acute pandysautonomia? Neurology. 1993; 43:132–137. doi: 10.1212/wnl.43.1_part_1.132 - PubMed
-
- Grubb BP, Kosinski DJ, Boehm K, Kip K. The postural orthostatic tachycardia syndrome: a neurocardiogenic variant identified during head-up tilt table testing. Pacing Clin Electrophysiol. 1997; 209 Pt 12205–2212. doi: 10.1111/j.1540-8159.1997.tb04238.x - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
