

Accuracy and Workflow Improvements for Responsive Neurostimulation Hippocampal Depth Electrode Placement Using Robotic Stereotaxy
- PMID: 33424745
- PMCID: PMC7793880
- DOI: 10.3389/fneur.2020.590825
Accuracy and Workflow Improvements for Responsive Neurostimulation Hippocampal Depth Electrode Placement Using Robotic Stereotaxy
Abstract
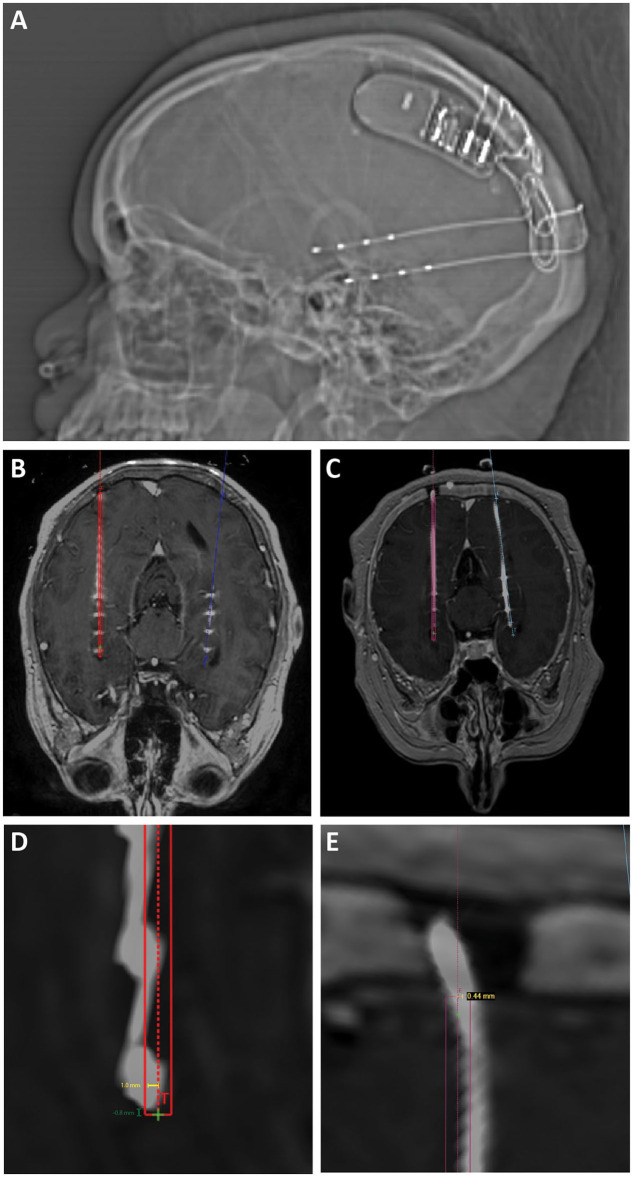
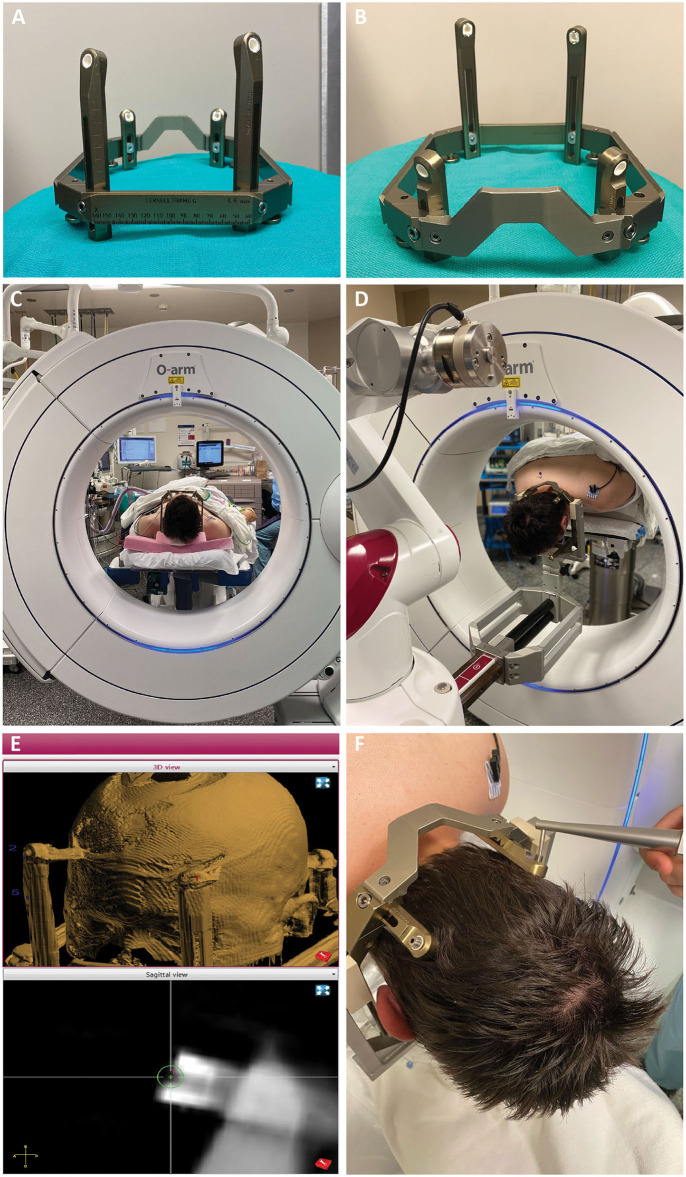
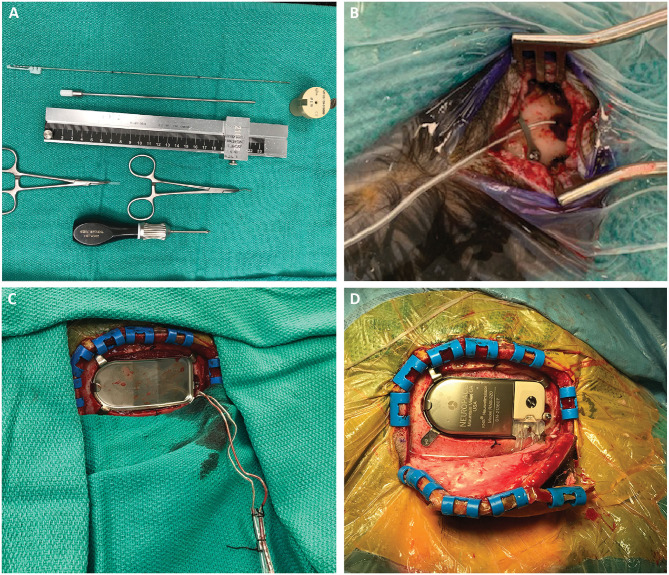
Background: Robotic stereotaxy is increasingly common in epilepsy surgery for the implantation of stereo-electroencephalography (sEEG) electrodes for intracranial seizure monitoring. The use of robots is also gaining popularity for permanent stereotactic lead implantation applications such as in deep brain stimulation and responsive neurostimulation (RNS) procedures. Objective: We describe the evolution of our robotic stereotactic implantation technique for placement of occipital-approach hippocampal RNS depth leads. Methods: We performed a retrospective review of 10 consecutive patients who underwent robotic RNS hippocampal depth electrode implantation. Accuracy of depth lead implantation was measured by registering intraoperative post-implantation fluoroscopic CT images and post-operative CT scans with the stereotactic plan to measure implantation accuracy. Seizure data were also collected from the RNS devices and analyzed to obtain initial seizure control outcome estimates. Results: Ten patients underwent occipital-approach hippocampal RNS depth electrode placement for medically refractory epilepsy. A total of 18 depth electrodes were included in the analysis. Six patients (10 electrodes) were implanted in the supine position, with mean target radial error of 1.9 ± 0.9 mm (mean ± SD). Four patients (8 electrodes) were implanted in the prone position, with mean radial error of 0.8 ± 0.3 mm. The radial error was significantly smaller when electrodes were implanted in the prone position compared to the supine position (p = 0.002). Early results (median follow-up time 7.4 months) demonstrate mean seizure frequency reduction of 26% (n = 8), with 37.5% achieving ≥50% reduction in seizure frequency as measured by RNS long episode counts. Conclusion: Prone positioning for robotic implantation of occipital-approach hippocampal RNS depth electrodes led to lower radial target error compared to supine positioning. The robotic platform offers a number of workflow advantages over traditional frame-based approaches, including parallel rather than serial operation in a bilateral case, decreased concern regarding human error in setting frame coordinates, and surgeon comfort.
Keywords: NeuroPace; RNS workflow; hippocampal depth electrode; responsive neurostimulation (RNS); robotic stereotaxy; robotic stereotaxy accuracy.
Copyright © 2020 Karas, Giridharan, Treiber, Prablek, Khan, Shofty, Krishnan, Chu, Van Ness, Maheshwari, Haneef, Gavvala and Sheth.
Conflict of interest statement
SS is a consultant for Boston Scientific, Abbott, and Zimmer Biomet. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Youngerman BE, Oh JY, Anbarasan D, Billakota S, Casadei CH, Corrigan EK, et al. . Laser ablation is effective for temporal lobe epilepsy with and without mesial temporal sclerosis if hippocampal seizure onsets are localized by stereoelectroencephalography. Epilepsia. (2018) 59:595–606. 10.1111/epi.14004 - DOI - PubMed
-
- Karas PJ, Sheth SA, Yoshor D. Epilepsy: mesial temporal. In: Pouratian N, Sheth SA, editors. Stereotactic and Functional Neurosurgery: Principles and Applications. Cham: Springer International Publishing; (2020). p. 339–67.
LinkOut - more resources
Full Text Sources