

Early Supported Discharge for Neurorehabilitation Following Acquired Brain Injury
- PMID: 33424748
- PMCID: PMC7793829
- DOI: 10.3389/fneur.2020.596526
Early Supported Discharge for Neurorehabilitation Following Acquired Brain Injury
Abstract
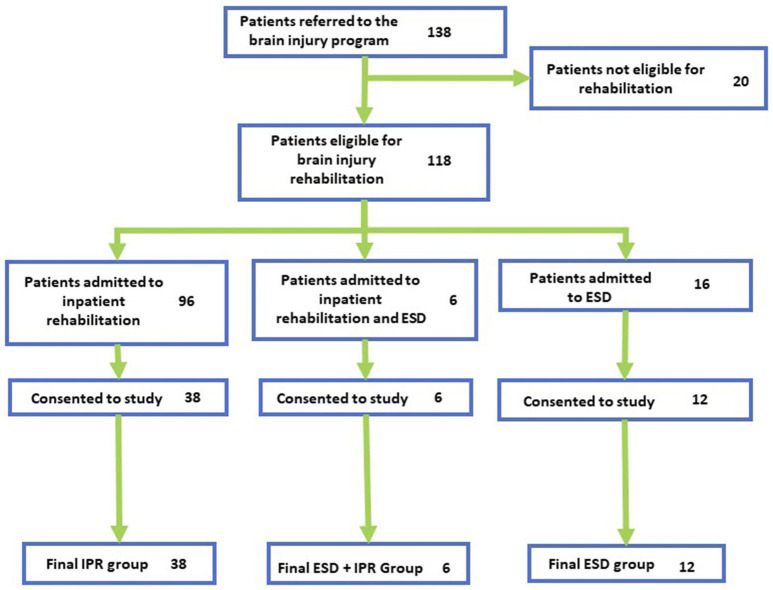
Introduction: Early Supported Discharge (ESD) is a clinical flow management service offering interdisciplinary rehabilitation, wherein patients are provided supported in-home rehabilitation treatment; in comparison to conventional hospital-based rehabilitation model of service delivery. There has been little research into the functional outcomes for other types of acquired brain injury (ABI). Methods: In this prospective cohort study, ABI patients presenting at a level I trauma center in Calgary, Canada were placed in either an ESD program or conventional inpatient rehabilitation (IPR) program based on their medical history and presentation. A small number of patients completed both programs (ESD+IPR group). ESD therapies were designed to emulate IPR. Participants completed professionally-rated Mayo-Portland Adaptability Index-4 (MPAI), Quality of Life after Brain Injury (QOLIBRI), Generalized Anxiety Questionnaire-7 (GAD7), Montreal Cognitive Assessment (MoCA), and Patient Health Questionnaire-9 (PHQ9) surveys at 1, 3, and 6 months following initial assessment pre-rehabilitation. Caregivers completed the Zarit Burden Interview (ZBI) at the same time points. The Supervision Rating Scale (SRS) and Disability Rating Scale (DRS) were completed at admission to rehabilitation and all follow-ups. Generalized estimate equations models were used to describe the three groups over time, including age as a covariate. Results: Significant effects of time were reported in the MPAI participant sub-score in the ESD and IPR groups ( = 42.429, p < 0.000; = 9.773, p = 0.008), showing significantly higher scores between 1 and 3 month timepoints for both groups. ZBI scores were significantly lower in the ESD group at 1 month compared to 3 and 6 months ( = 31.252, p < 0.001). The proportion of patients with medical complications during rehabilitation was 25.3% in ESD compared to 74.7% patients in IPR. Conclusions: Improvements in functional outcomes were evident in patients participating in ESD and IPR, with more medical complications reported in the IPR group. Caregiver burden lessened over time in the ESD group but not in the IPR group. Both ESD and ESD+IPR groups can be considered viable alternatives to traditional inpatient rehabilitation. A randomized control trial would be required to properly compare rehabilitation streams. Further investigation into affective and lifestyle elements of ABI recovery would also improve our understanding of targeted neurorehabilitation in this population.
Keywords: acquired brain injured (ABI); caregiver burden; early supported discharge (ESD); functional outcome; in-home rehabilitation; neurorehabiliation.
Copyright © 2020 King, Seeger, Wang, Li Pi Shan, McGovern, Knox, Patel, Fung, Sajobi and Debert.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
An Observational Cohort Study of the Role of Level of Effort in Post-Acute Brain Injury Rehabilitation.Arch Phys Med Rehabil. 2023 Feb;104(2):211-217. doi: 10.1016/j.apmr.2022.07.013. Epub 2022 Aug 5. Arch Phys Med Rehabil. 2023. PMID: 35934046
-
Evaluation of Posthospital Brain Injury Rehabilitation Outcomes With Quasi-Experimental Controls.J Head Trauma Rehabil. 2025 Jan-Feb 01;40(1):38-45. doi: 10.1097/HTR.0000000000000993. Epub 2024 Aug 5. J Head Trauma Rehabil. 2025. PMID: 39103287
-
Outcomes of Six Specific Types of Post-Hospital Brain Injury Rehabilitation Programs.J Head Trauma Rehabil. 2025 Jan-Feb 01;40(1):27-37. doi: 10.1097/HTR.0000000000000980. Epub 2024 Jun 24. J Head Trauma Rehabil. 2025. PMID: 38916445
-
Does self-awareness influence caregiver burden?NeuroRehabilitation. 2020;46(4):511-518. doi: 10.3233/NRE-203093. NeuroRehabilitation. 2020. PMID: 32538884
-
Evidence reviews for early supported discharge: Stroke rehabilitation in adults (update): Evidence review A1.London: National Institute for Health and Care Excellence (NICE); 2023 Oct. London: National Institute for Health and Care Excellence (NICE); 2023 Oct. PMID: 38359154 Free Books & Documents. Review.
Cited by
-
Rehabilitation models that support transitions from hospital to home for people with acquired brain injury (ABI): a scoping review.BMC Health Serv Res. 2023 Jul 31;23(1):814. doi: 10.1186/s12913-023-09793-x. BMC Health Serv Res. 2023. PMID: 37525270 Free PMC article.
-
The Measure of an Outcome: Comparing Norming and Stacking to Benchmark the Effectiveness of Brain Injury Rehabilitation Services.Behav Sci (Basel). 2023 Aug 25;13(9):705. doi: 10.3390/bs13090705. Behav Sci (Basel). 2023. PMID: 37753983 Free PMC article.
-
Factors influencing the implementation of early discharge hospital at home and admission avoidance hospital at home: a qualitative evidence synthesis.Cochrane Database Syst Rev. 2024 Mar 5;3(3):CD014765. doi: 10.1002/14651858.CD014765.pub2. Cochrane Database Syst Rev. 2024. PMID: 38438114 Free PMC article.
-
Investigating the effects of home-based rehabilitation after intensive inpatient rehabilitation on motor function, activities of daily living, and caregiver burden.PLoS One. 2024 Dec 27;19(12):e0316163. doi: 10.1371/journal.pone.0316163. eCollection 2024. PLoS One. 2024. PMID: 39729469 Free PMC article.
References
-
- Finnanger TG, Olsen A, Skandsen T, Lydersen S, Vik A, Evensen KA, et al. . Life after adolescent and adult moderate and severe traumatic brain injury: self-reported executive, emotional, and behavioural function 2-5 years after injury. Behav Neurol. (2015) 2015:329241.10.1155/2015/329241 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous