

Pro-inflammatory dopamine-2 receptor-specific T cells in paediatric movement and psychiatric disorders
- PMID: 33425355
- PMCID: PMC7780098
- DOI: 10.1002/cti2.1229
Pro-inflammatory dopamine-2 receptor-specific T cells in paediatric movement and psychiatric disorders
Abstract
Objectives: A dysregulated inflammatory response against the dopamine-2 receptor (D2R) has been implicated in movement and psychiatric disorders. D2R antibodies were previously reported in a subset of these patients; however, the role of T cells in these disorders remains unknown. Our objective was to identify and characterise pro-inflammatory D2R-specific T cells in movement and psychiatric disorders.
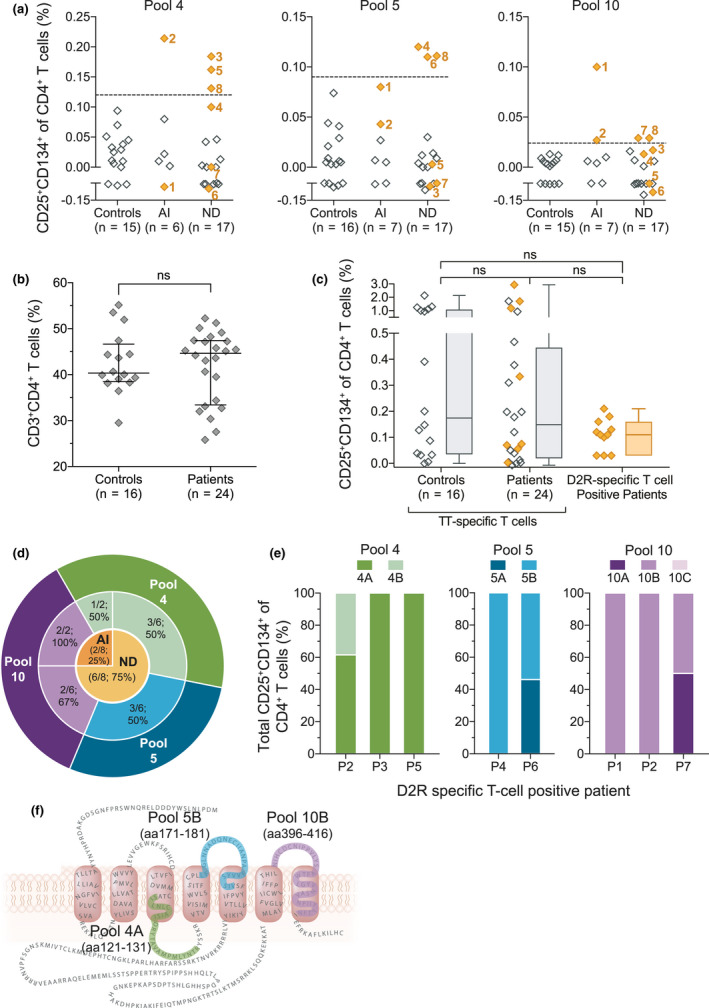
Methods: Blood from paediatric patients with movement and psychiatric disorders of suspected autoimmune and neurodevelopmental aetiology (n = 24) and controls (n = 16) was cultured in vitro with a human D2R peptide library, and D2R-specific T cells were identified by flow cytometric quantification of CD4+CD25+CD134+ T cells. Cytokine secretion was analysed using a cytometric bead array and ELISA. HLA genotypes were examined in D2R-specific T-cell-positive patients. D2R antibody seropositivity was determined using a flow cytometry live cell-based assay.
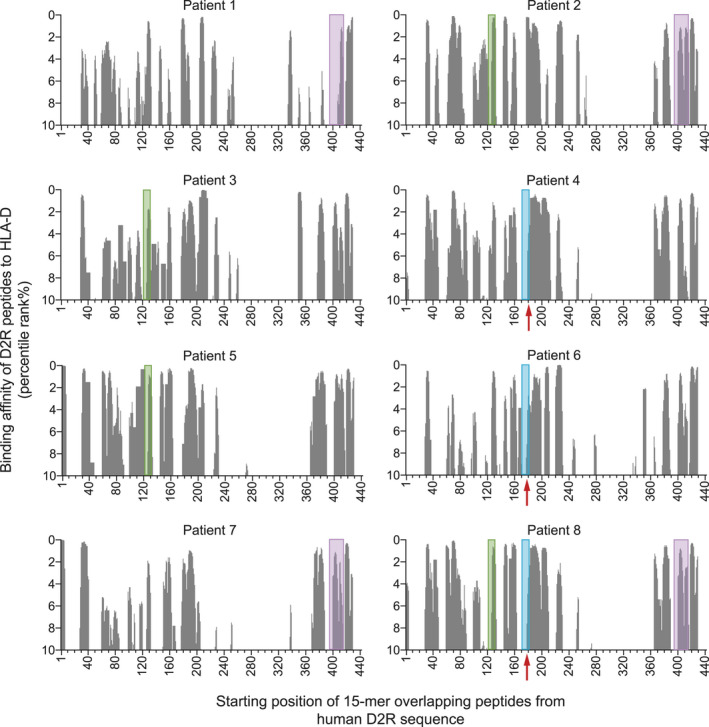
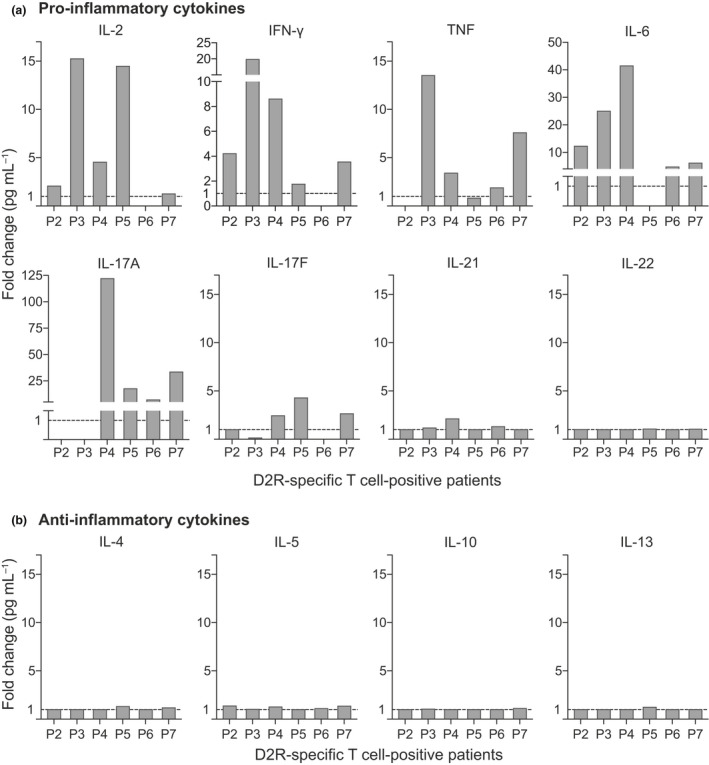
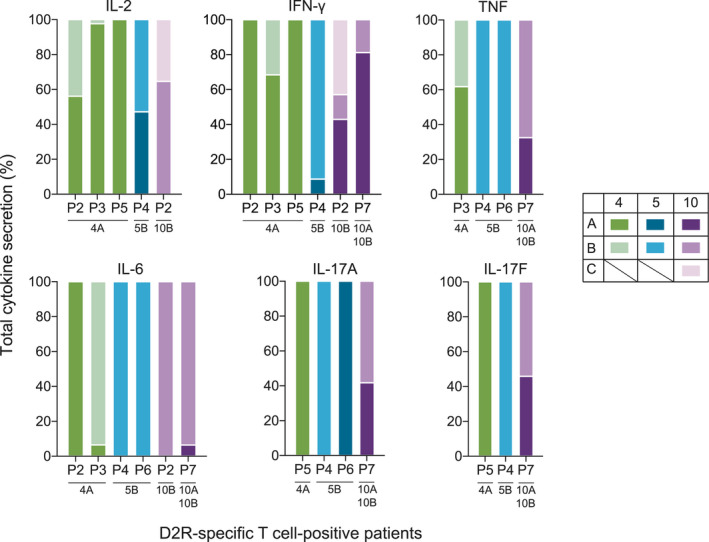
Results: Three immunodominant regions of D2R, amino acid (aa)121-131, aa171-181 and aa396-416, specifically activated CD4+ T cells in 8/24 patients. Peptides corresponding to these regions were predicted to bind with high affinity to the HLA of the eight positive patients and had also elicited the secretion of pro-inflammatory cytokines IL-2, IFN- γ, TNF, IL-6, IL-17A and IL-17F. All eight patients were seronegative for D2R antibodies.
Conclusion: Autoreactive D2R-specific T cells and a pro-inflammatory Th1 and Th17 cytokine profile characterise a subset of paediatric patients with movement and psychiatric disorders, further underpinning the theory of immune dysregulation in these disorders. These findings offer new perspectives into the neuroinflammatory mechanisms of movement and psychiatric disorders and can influence patient diagnosis and treatment.
Keywords: autoimmune encephalitis; autoimmunity; dopamine‐2 receptor antibodies; neurodevelopmental disorders; pro‐inflammatory T cells.
© 2020 The Authors. Clinical & Translational Immunology published by John Wiley & Sons Australia, Ltd on behalf of Australian and New Zealand Society for Immunology Inc.
Conflict of interest statement
DP reports funding from the Neville Brown Scholarship (Australia). SR reports fellowship research funding from the National Health and Medical Research Council (Australia). RCD and FB have received research funding from the Trish Multiple Sclerosis Research Foundation, Multiple Sclerosis Research Australia, the Petre Foundation and the National Health Medical Research Council (Australia). They have received honoraria from Biogen Idec and Merck Serono as invited speakers. AZ, RD, JAL, FT, GL, FXZL, VM, SDH, AP, HFJ, SM, ADK and SIA declare no competing interests.
Figures
References
-
- Dalmau J, Graus F. Antibody‐mediated encephalitis. N Engl J Med 2018; 378: 840–851. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials