

Diffuse Recurrence of Hepatocellular Carcinoma After Liver Resection: Transarterial Chemoembolization (TACE) Combined With Sorafenib Versus TACE Monotherapy
- PMID: 33425729
- PMCID: PMC7793644
- DOI: 10.3389/fonc.2020.574668
Diffuse Recurrence of Hepatocellular Carcinoma After Liver Resection: Transarterial Chemoembolization (TACE) Combined With Sorafenib Versus TACE Monotherapy
Abstract
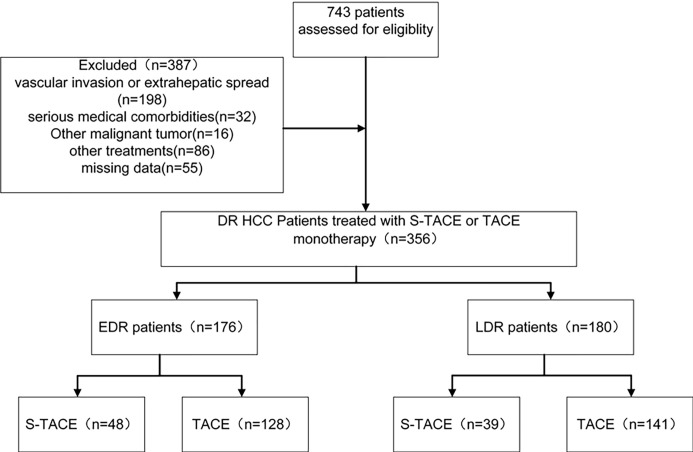
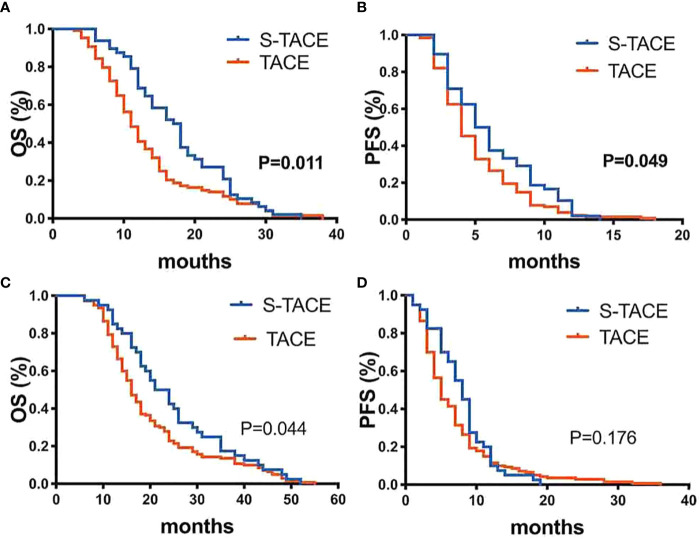
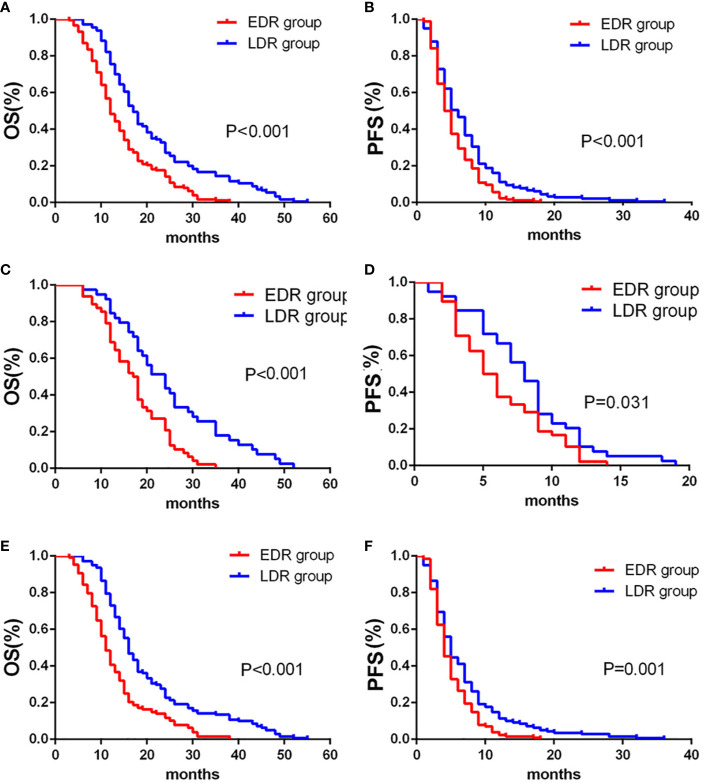
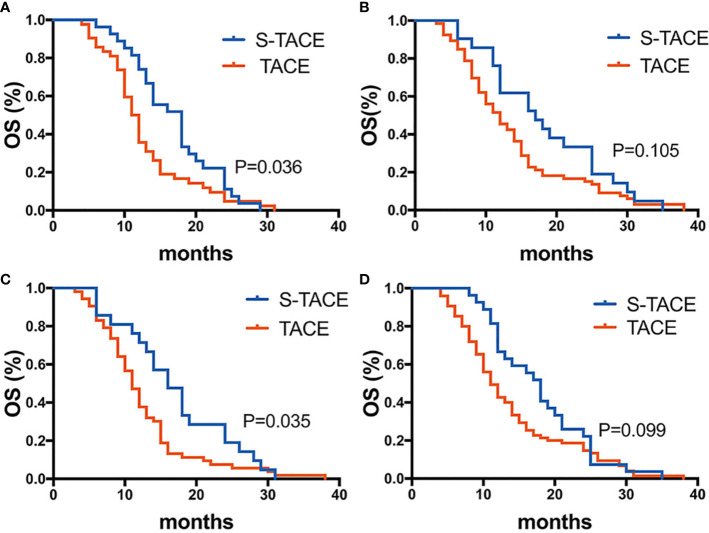
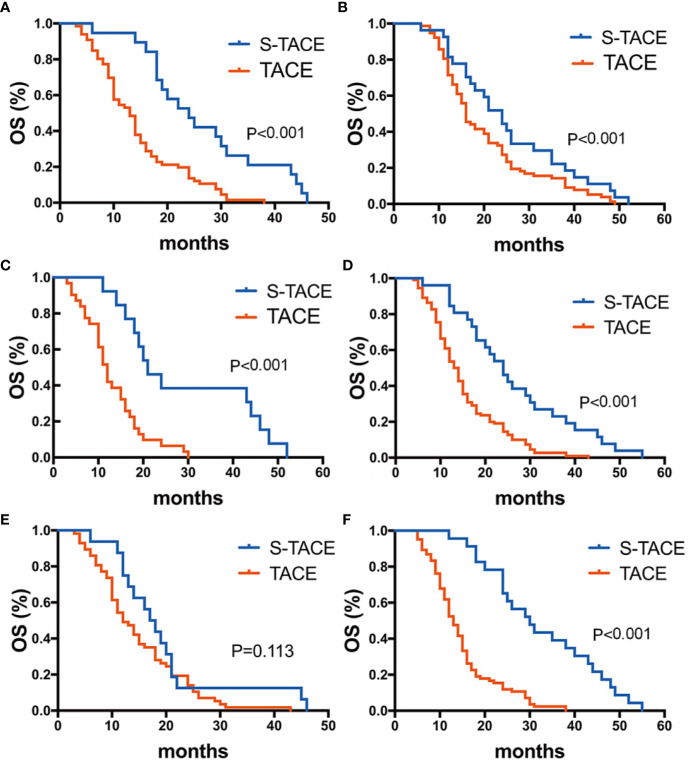
This study aims to compare the effectiveness and complications of transarterial chemoembolization (TACE) combined with sorafenib (S-TACE) and TACE monotherapy in HCC patients with diffuse recurrence (DR). This retrospective study was approved by our hospital ethics committee, and all patients provided informed consent. We retrospectively enrolled 356 DR patients from January 2005 to December 2014, who underwent either S-TACE or TACE monotherapy. Treatment complications, overall survival (OS) and progression-free survival (PFS) were evaluated. Survival curves were constructed using the Kaplan-Meier method and compared using a log-rank test. Our results found a significant difference between S-TACE and TACE monotherapy in the PFS and OS of HCC patients with early diffuse recurrence (EDR) (p=0.011 and 0.049, respectively). Patients with late diffuse recurrence (LDR) who underwent S-TACE had longer OS (median 24.0 vs. 16.0 months; p=0.044) compared with those in the TACE monotherapy group. Subgroup analysis revealed that S-TACE therapy resulted in higher OS of EDR patients with tumors > 5 cm and HBV-DNA >100 (p=0.036 and 0.035, respectively), compared with patients given TACE monotherapy. S-TACE therapy also resulted in better OS in LDR patients with AFP≥400 ng/ml, AFP<400 ng/ml, TB<28 g/L, TB>28 g/L, and a maximum tumor diameter < 5 cm (p=<0.001, 0.042, <0.001, <0.001, and <0.001, respectively). The rate of major complications in patients who underwent S-TACE was not significantly different to those who underwent TACE monotherapy (33.5% vs. 28.2%, p= 0.69). Overall, patients given S-TACE had better OS in both EDR and LDR patients, but only EDR patients had better PFS.
Keywords: diffuse recurrence; hepatocellular carcinoma; liver resection; sorafenib; transarterial chemoembolization.
Copyright © 2020 Yao, Xue, Lu, Wang, Zhao, Wu, Fan and Li.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Microvascular Invasion as a Predictor of Response to Treatment with Sorafenib and Transarterial Chemoembolization for Recurrent Intermediate-Stage Hepatocellular Carcinoma.Radiology. 2019 Jul;292(1):237-247. doi: 10.1148/radiol.2019181818. Epub 2019 May 28. Radiology. 2019. PMID: 31135299
-
Transarterial chemoembolization (TACE) combined with apatinib versus TACE combined with sorafenib in advanced hepatocellular carcinoma patients: a multicenter retrospective study.Ann Transl Med. 2021 Feb;9(4):283. doi: 10.21037/atm-20-5360. Ann Transl Med. 2021. PMID: 33708910 Free PMC article.
-
Large primary hepatocellular carcinoma: transarterial chemoembolization monotherapy versus combined transarterial chemoembolization-percutaneous microwave coagulation therapy.J Gastroenterol Hepatol. 2013 Mar;28(3):456-63. doi: 10.1111/jgh.12088. J Gastroenterol Hepatol. 2013. PMID: 23216261
-
Transarterial chemoembolization combined with lenvatinib versus transarterial chemoembolization combined with sorafenib for unresectable hepatocellular carcinoma: A comparative retrospective study.Hepatol Res. 2022 Sep;52(9):794-803. doi: 10.1111/hepr.13801. Epub 2022 Jun 30. Hepatol Res. 2022. PMID: 35698267
-
Transarterial chemoembolization versus hepatic resection in hepatocellular carcinoma treatment: a meta-analysis.Drug Des Devel Ther. 2015 Aug 10;9:4431-40. doi: 10.2147/DDDT.S86629. eCollection 2015. Drug Des Devel Ther. 2015. PMID: 26309396 Free PMC article. Review.
Cited by
-
The efficacy and safety of lenvatinib plus transarterial chemoembolization in combination with PD-1 antibody in treatment of unresectable recurrent hepatocellular carcinoma: a case series report.Front Oncol. 2023 May 16;13:1096955. doi: 10.3389/fonc.2023.1096955. eCollection 2023. Front Oncol. 2023. PMID: 37260972 Free PMC article.
-
Novel Microcrystal Formulations of Sorafenib Facilitate a Long-Acting Antitumor Effect and Relieve Treatment Side Effects as Observed With Fundus Microcirculation Imaging.Front Oncol. 2021 Aug 26;11:743055. doi: 10.3389/fonc.2021.743055. eCollection 2021. Front Oncol. 2021. PMID: 34513717 Free PMC article.
-
Transarterial Chemoembolization for Hepatocellular Carcinoma: Why, When, How?J Pers Med. 2022 Mar 10;12(3):436. doi: 10.3390/jpm12030436. J Pers Med. 2022. PMID: 35330436 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous