

Acute Kidney Injury Associated With Urinary Stone Disease in Children and Young Adults Presenting to a Pediatric Emergency Department
- PMID: 33425812
- PMCID: PMC7793999
- DOI: 10.3389/fped.2020.591520
Acute Kidney Injury Associated With Urinary Stone Disease in Children and Young Adults Presenting to a Pediatric Emergency Department
Abstract
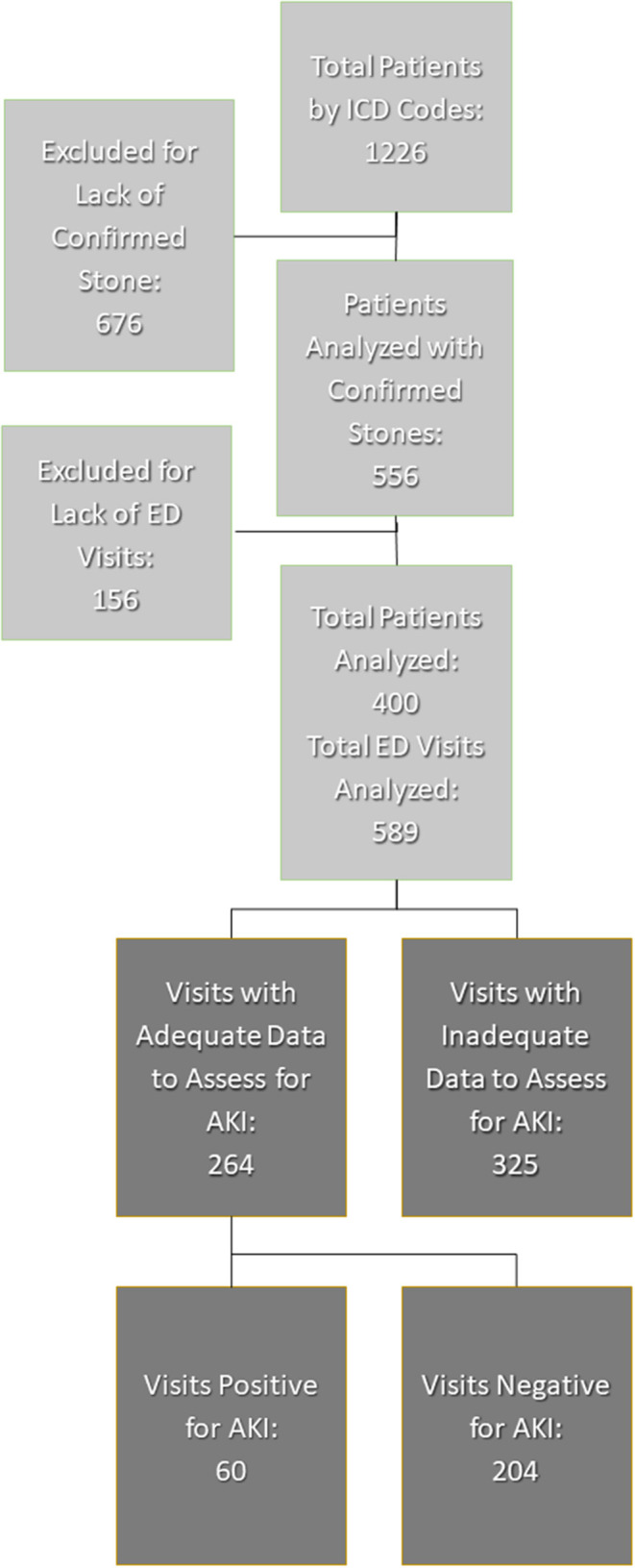
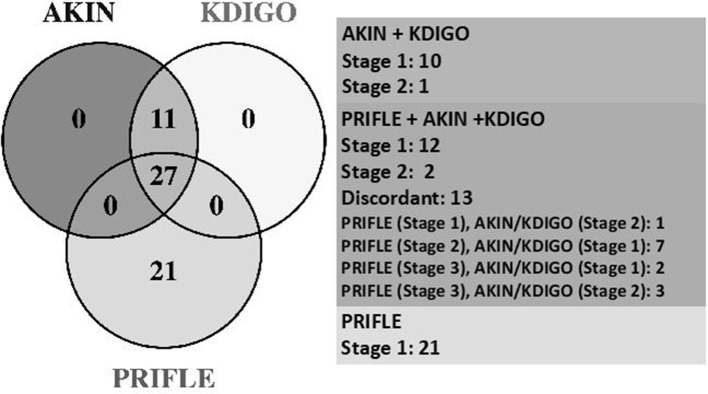
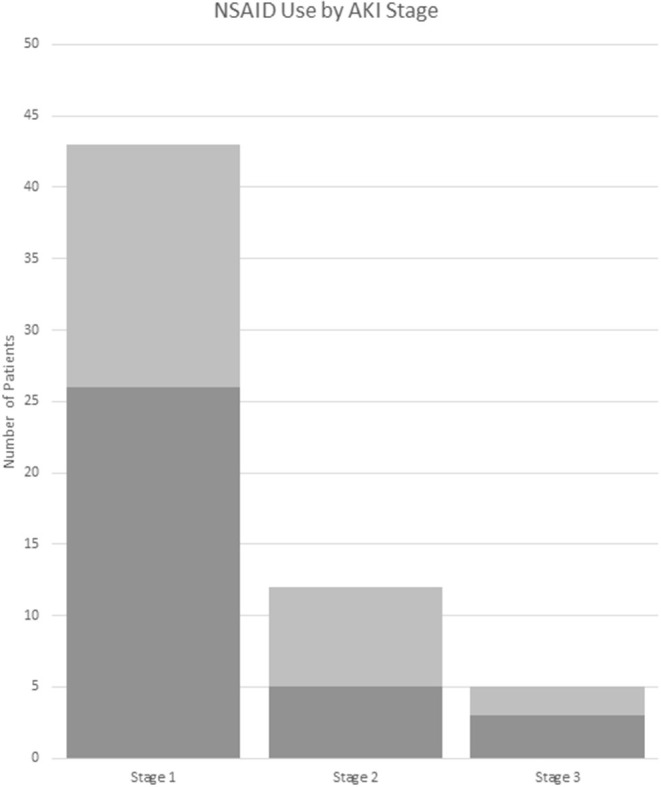
Background: Acute kidney injury (AKI) due to urinary stone disease (USD) is rare in adults; AKI rates in children with USD may be higher, and emerging data links stones to chronic kidney disease (CKD) development in adults. Methods: This study is a retrospective analysis of USD patients at a single pediatric hospital system's emergency department (ED). Patients were initially identified by USD ICD codes; USD was then confirmed by imaging or physician documentation; patients had to have baseline creatinine (Cr) and Cr in the ED for comparison to be included. AKI was defined by Kidney Disease: Improving Global Outcomes (KDIGO), Acute Kidney Injury Network (AKIN), and Pediatric Risk, Injury, Failure, Loss, End Stage (pRIFLE). Results: Of the 589 total visits, 264/589 (45%) had data to evaluate for AKI, 23% were AKI(+) and 77% were AKI(-). pRIFLE was most common (82%) and 18% were only positive by AKIN/KDIGO. AKI(+) were more likely to be younger (16.7 vs. 17.4 years, p = 0.046) and more likely to present with vomiting {odds ratio [OR] [95% confidence interval (CI)]: 2.4 [1.4-4.3], p = 0.002}; also, the proportion of AKI(+) was significantly higher in <18 vs. ≥18 years [26.9 vs. 15.5%, p = 0.032, OR (95% CI): 2.0 (1.1-3.9)]. Urinary tract infection (UTI) and obstruction rates were similar between groups. AKI(+) patients had a significant OR <1 suggesting less risk of receiving non-steroidal anti-inflammatory drugs (NSAIDs); however, 51% of them did receive NSAIDs during their ED encounter. AKI(+) patients were more likely to require admission to the hospital (53 vs. 32%, p = 0.001). Conclusion: We have demonstrated a novel association between USD-induced renal colic and AKI in a group of young adults and children. AKI(+) patients were younger and were more likely to present with vomiting. AKI(+) patients did not have higher rates of obstruction or UTI, and 51% of AKI(+) received NSAIDs.
Keywords: AKI; kidney stones; pediatric; urinary stone disease (USD); urolithiasis.
Copyright © 2020 Farris, Raina, Tibrewal, Brown, Colvis, Schwaderer and Kusumi.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
A comparison of the systems for the identification of postoperative acute kidney injury in pediatric cardiac patients.Ann Thorac Surg. 2014 Jan;97(1):202-10. doi: 10.1016/j.athoracsur.2013.09.014. Epub 2013 Nov 6. Ann Thorac Surg. 2014. PMID: 24206964
-
Acute kidney injury in congenital cardiac surgery: Pediatric risk-injury-failure-loss-end-stage renal disease and Acute Kidney Injury Network.Pediatr Int. 2017 Dec;59(12):1252-1260. doi: 10.1111/ped.13359. Pediatr Int. 2017. PMID: 28672079
-
Incidence, admission rates, and economic burden of pediatric emergency department visits for urinary tract infection: data from the nationwide emergency department sample, 2006 to 2011.J Pediatr Urol. 2015 Oct;11(5):246.e1-8. doi: 10.1016/j.jpurol.2014.10.005. Epub 2015 Feb 7. J Pediatr Urol. 2015. PMID: 26005017
-
Incidence of Antimicrobial-Associated Acute Kidney Injury in Children: A Structured Review.Paediatr Drugs. 2024 Jan;26(1):59-70. doi: 10.1007/s40272-023-00607-5. Epub 2023 Dec 13. Paediatr Drugs. 2024. PMID: 38093147 Free PMC article. Review.
-
Epidemiology of acute kidney injury in children worldwide, including developing countries.Pediatr Nephrol. 2017 Aug;32(8):1301-1314. doi: 10.1007/s00467-016-3433-2. Epub 2016 Jun 15. Pediatr Nephrol. 2017. PMID: 27307245 Review.
Cited by
-
Urinary stone disease in Syrian children.Pediatr Nephrol. 2023 Aug;38(8):2699-2709. doi: 10.1007/s00467-022-05860-3. Epub 2023 Jan 20. Pediatr Nephrol. 2023. PMID: 36662300
-
Development and validation of a predictive model for acute kidney injury in patients with ureterolithiasis.Ren Fail. 2024 Dec;46(2):2394634. doi: 10.1080/0886022X.2024.2394634. Epub 2024 Aug 23. Ren Fail. 2024. PMID: 39177235 Free PMC article.
-
Clinical characteristics and outcomes of children with hypertensive encephalopathy.BMC Pediatr. 2025 Jul 17;25(1):558. doi: 10.1186/s12887-025-05909-w. BMC Pediatr. 2025. PMID: 40676587 Free PMC article.
References
LinkOut - more resources
Full Text Sources