

Hemostatic Balance in Pediatric Acute Liver Failure: Epidemiology of Bleeding and Thrombosis, Physiology, and Current Strategies
- PMID: 33425821
- PMCID: PMC7786276
- DOI: 10.3389/fped.2020.618119
Hemostatic Balance in Pediatric Acute Liver Failure: Epidemiology of Bleeding and Thrombosis, Physiology, and Current Strategies
Abstract
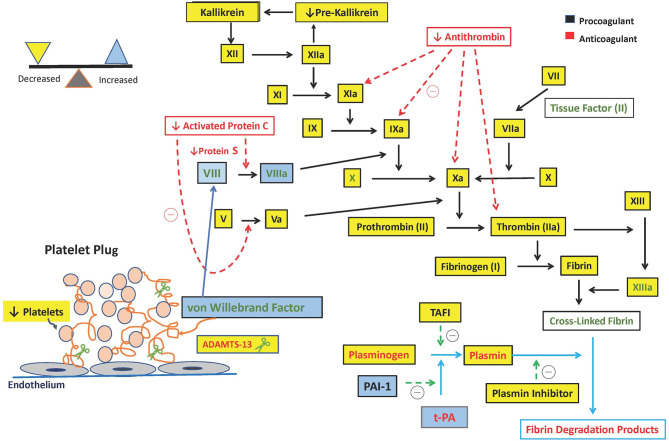
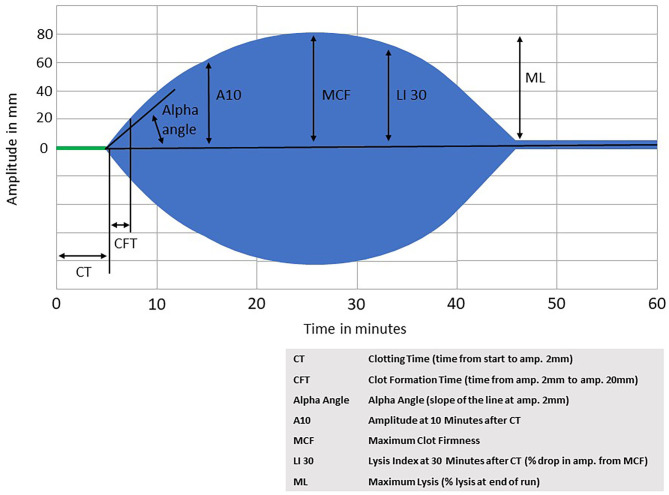
Pediatric Acute Liver Failure (PALF) is a rapidly progressive clinical syndrome encountered in the pediatric ICU which may rapidly progress to multi-organ dysfunction, and on occasion to life threatening cerebral edema and hemorrhage. Pediatric Acute Liver Failure is defined as severe acute hepatic dysfunction accompanied by encephalopathy and liver-based coagulopathy defined as prolongation of International Normalized Ratio (INR) >1.5. However, coagulopathy in PALF is complex and warrants a deeper understanding of the hemostatic balance in acute liver failure. Although an INR value of >1.5 is accepted as the evidence of coagulopathy and has historically been viewed as a prognostic factor of PALF, it may not accurately reflect the bleeding risk in PALF since it only measures procoagulant factors. Paradoxically, despite the prolongation of INR, bleeding risk is lower than expected (around 5%). This is due to "rebalanced hemostasis" due to concurrent changes in procoagulant, anticoagulant and fibrinolytic systems. Since the liver is involved in both procoagulant (Factors II, V, IX, XI, and fibrinogen) and anticoagulant (Protein C, Protein S, and antithrombin) protein synthesis, PALF results in "rebalanced hemostasis" or even may shift toward a hypercoagulable state. In addition to rebalanced coagulation there is altered platelet production due to decreased thrombopoietin production by liver, increased von Willebrand factor from low grade endothelial cell activation, and hyperfibrinolysis and dysfibrinogenemia from altered synthetic liver dysfunction. All these alterations contribute to the multifactorial nature of coagulopathy in PALF. Over exuberant use of prophylactic blood products in patients with PALF may contribute to morbidities such as fluid overload, transfusion-associated lung injury, and increased thrombosis risk. It is essential to use caution when using INR values for plasma and factor administration. In this review we will summarize the complexity of coagulation in PALF, explore "rebalanced hemostasis," and discuss the limitations of current coagulation tests. We will also review strategies to accurately diagnose the coagulopathy of PALF and targeted therapies.
Keywords: PALF; children; coagulopathy; critical care; hemostasis; liver failure; thrombosis; transfusion.
Copyright © 2020 Bulut, Sapru and Roach.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
AGA Clinical Practice Update: Coagulation in Cirrhosis.Gastroenterology. 2019 Jul;157(1):34-43.e1. doi: 10.1053/j.gastro.2019.03.070. Epub 2019 Apr 12. Gastroenterology. 2019. PMID: 30986390 Review.
-
Coagulopathy in liver disease: a balancing act.Hematology Am Soc Hematol Educ Program. 2015;2015:243-9. doi: 10.1182/asheducation-2015.1.243. Hematology Am Soc Hematol Educ Program. 2015. PMID: 26637729
-
Hemostasis in liver transplantation: Pathophysiology, monitoring, and treatment.World J Gastroenterol. 2016 Jan 28;22(4):1541-50. doi: 10.3748/wjg.v22.i4.1541. World J Gastroenterol. 2016. PMID: 26819521 Free PMC article. Review.
-
Viscoelastic tests in liver disease: where do we stand now?World J Gastroenterol. 2021 Jun 21;27(23):3290-3302. doi: 10.3748/wjg.v27.i23.3290. World J Gastroenterol. 2021. PMID: 34163112 Free PMC article. Review.
-
Critical issues in hematology: anemia, thrombocytopenia, coagulopathy, and blood product transfusions in critically ill patients.Clin Chest Med. 2003 Dec;24(4):607-22. doi: 10.1016/s0272-5231(03)00100-x. Clin Chest Med. 2003. PMID: 14710693 Review.
Cited by
-
Is there a role for extracorporeal membrane oxygenation in children with acute liver failure? A retrospective analysis of the Extracorporeal Life Support Organization Registry.Eur J Pediatr. 2024 Nov;183(11):5013-5019. doi: 10.1007/s00431-024-05794-y. Epub 2024 Sep 25. Eur J Pediatr. 2024. PMID: 39322851
-
Pediatric thrombosis: Risk factors, diagnosis, and prevention strategies.Medicine (Baltimore). 2025 Jul 18;104(29):e43370. doi: 10.1097/MD.0000000000043370. Medicine (Baltimore). 2025. PMID: 40696594 Free PMC article. Review.
-
Severe acute hepatitis of unknown etiology in children in 2022: A Narrative Review.New Microbes New Infect. 2023 Jan 21;51:101087. doi: 10.1016/j.nmni.2023.101087. eCollection 2023 Jan. New Microbes New Infect. 2023. PMID: 36755794 Free PMC article. Review.
-
[Advancements in the diagnosis and treatment of pediatric acute liver failure].Zhongguo Dang Dai Er Ke Za Zhi. 2024 Feb 15;26(2):194-200. doi: 10.7499/j.issn.1008-8830.2309015. Zhongguo Dang Dai Er Ke Za Zhi. 2024. PMID: 38436319 Free PMC article. Review. Chinese.
-
Establishment of a risk assessment score for deep vein thrombosis after artificial liver support system treatment.World J Clin Cases. 2021 Nov 6;9(31):9406-9416. doi: 10.12998/wjcc.v9.i31.9406. World J Clin Cases. 2021. PMID: 34877276 Free PMC article.
References
-
- Ewe K. Bleeding after liver biopsy does not correlate with indices of peripheral coagulation. Dig Dis Sci. (1981) 26(5):388-393. - PubMed
Publication types
LinkOut - more resources
Full Text Sources