

Case Report: ST-Segment Elevation in a Man With Acute Pericarditis
- PMID: 33426006
- PMCID: PMC7793765
- DOI: 10.3389/fcvm.2020.609691
Case Report: ST-Segment Elevation in a Man With Acute Pericarditis
Abstract
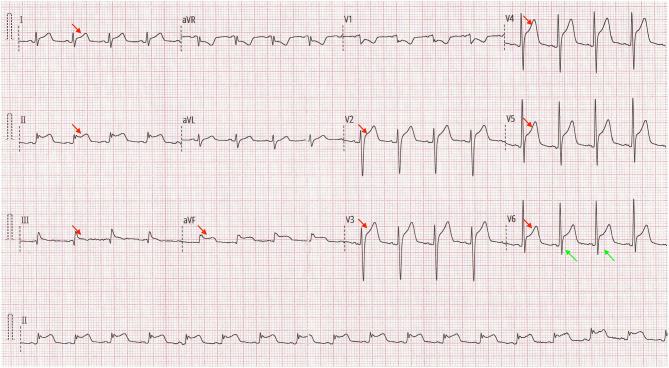
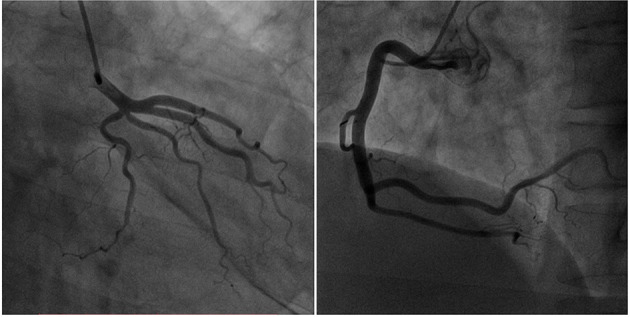
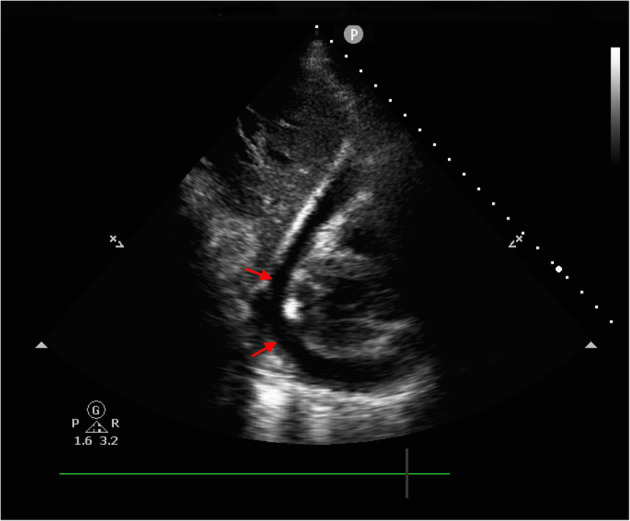
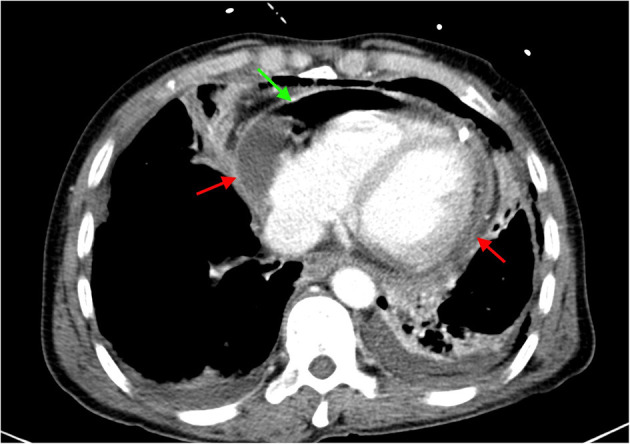
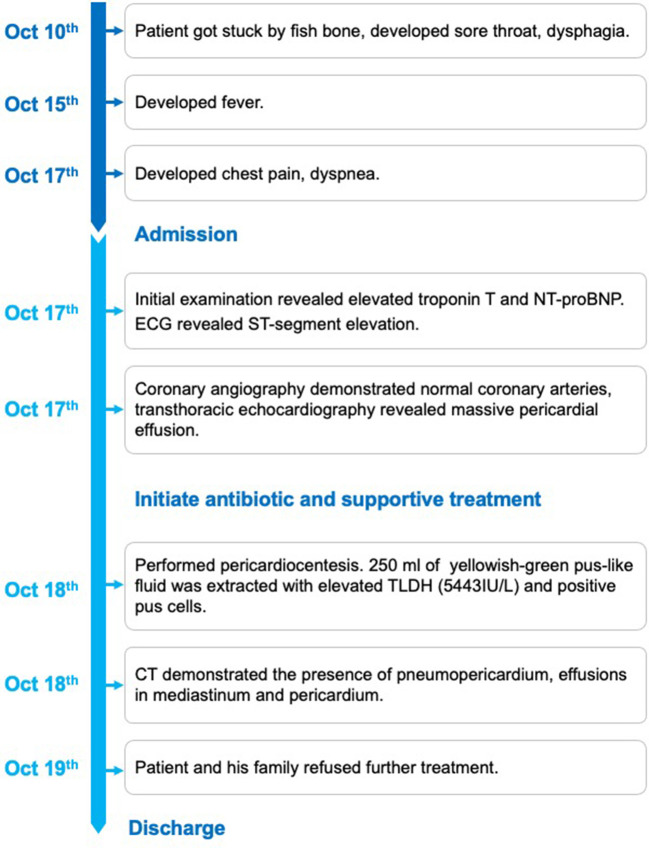
Background: Acute pericarditis is a rapid inflammatory condition of the pericardium with both infectious and non-infectious etiology. Most acute pericarditis is self-limited, with a small portion evolving rapidly. The definitive diagnosis of acute pericarditis often requires detailed physical examination, ECG, echocardiography, blood analysis and chest X-ray. It's usually challenging to distinguish acute pericarditis from ST-elevated myocardial infarction (STEMI) due to the similar ECG characteristics (ST segment change). Here we present a case of purulent pericarditis probably caused by esophageal perforation. Case: A 52 year-old male presented with chest pain and dyspnea for 16 h. ST-segment elevation and positive cardiac markers lead to the initial diagnosis of ST-elevated myocardial infarction. Coronary angiography demonstrated normal coronary artery, while transthoracic echocardiography (TTE) showed massive pericardial effusion. Then, pericardiocentesis was performed with 250 ml of yellowish-green pus-like fluid extracted. A detailed history examination revealed a week history of possible esophageal perforation caused by a fishbone. And a further computed tomography (CT) demonstrated the presence of pneumomediastinum, and effusions in mediastinum, which lead to the diagnosis of purulent pericarditis. However, the patient's family refused further treatment and the patient died soon after discharge. Conclusion: The differential diagnosis of chest pain should include acute pericarditis, which can be equally critical and fatal. And it's important to note the peculiar characteristics of acute pericarditis, which include concave and diffused ST-segment elevation, PR segment depression, and the ratio of ST-segment elevation to T wave >0.24 in lead V6. Moreover, comprehensive medical history and physical examination are crucial to the differential diagnosis of chest pain patients.
Keywords: ECG; STEMI; acute pericarditis; esophageal perforation; purulent pericarditis.
Copyright © 2020 Li, Jia, Tsauo, Wang and Peng.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
PR depression with multilead ST elevation and ST depression in aVR by left circumflex artery occlusion: How to differentiate from acute pericarditis.Ann Noninvasive Electrocardiol. 2020 Nov;25(6):e12752. doi: 10.1111/anec.12752. Epub 2020 Feb 21. Ann Noninvasive Electrocardiol. 2020. PMID: 32083371 Free PMC article.
-
The importance of the evolution of ST-T wave changes for differentiating acute pericarditis from myocardial ischemia.Cardiol Rev. 2004 May-Jun;12(3):138-40. doi: 10.1097/01.crd.0000110745.25012.ba. Cardiol Rev. 2004. PMID: 15078582
-
Purulent pericarditis-induced intracardiac perforation and infective endocarditis due to Parvimonas micra: a case report.Eur Heart J Case Rep. 2020 Dec 29;5(2):ytaa528. doi: 10.1093/ehjcr/ytaa528. eCollection 2021 Feb. Eur Heart J Case Rep. 2020. PMID: 33598614 Free PMC article.
-
Acute pericarditis.Am Fam Physician. 2007 Nov 15;76(10):1509-14. Am Fam Physician. 2007. PMID: 18052017 Review.
-
Electrocardiographic manifestations and differential diagnosis of acute pericarditis.Am Fam Physician. 1998 Feb 15;57(4):699-704. Am Fam Physician. 1998. PMID: 9490993 Review.
Cited by
-
Fish bone migration: complications, diagnostic challenges, and treatment strategies.World J Emerg Surg. 2025 Apr 23;20(1):35. doi: 10.1186/s13017-025-00611-9. World J Emerg Surg. 2025. PMID: 40269939 Free PMC article.
-
Persistent convex ST-segment elevation in a patient with a history of prior intracerebral haemorrhage.ESC Heart Fail. 2024 Jun;11(3):1777-1784. doi: 10.1002/ehf2.14703. Epub 2024 Feb 6. ESC Heart Fail. 2024. PMID: 38321818 Free PMC article.
-
Esophageal perforation mimicking an acute inferior myocardial infarction: a case report.J Thorac Dis. 2024 Nov 30;16(11):8117-8125. doi: 10.21037/jtd-24-1616. Epub 2024 Nov 21. J Thorac Dis. 2024. PMID: 39678903 Free PMC article.
-
Myopericarditis Mimicking an Acute MI.Cureus. 2023 Dec 25;15(12):e51069. doi: 10.7759/cureus.51069. eCollection 2023 Dec. Cureus. 2023. PMID: 38269221 Free PMC article.
-
Importance of ECG in the Diagnosis of Acute Pericarditis and Myocardial Infarction: A Review Article.Cureus. 2022 Oct 24;14(10):e30633. doi: 10.7759/cureus.30633. eCollection 2022 Oct. Cureus. 2022. PMID: 36426313 Free PMC article. Review.
References
-
- Emergency Department Patients With Chest Pain Writing Panal. Rybicki FJ, Udelson JE, Peacock WF, Goldhaber SZ, Isselbacher EM, et al. 2015 ACR/ACC/AHA/AATS/ACEP/ASNC/NASCI/SAEM/SCCT/SCMR/SCPC/SNMMI/STR/STS appropriate utilization of cardiovascular imaging in Emergency Department patients with chest pain: a joint document of the American College of Radiology Appropriateness Criteria Committee and the American College of Cardiology Appropriate Use Criteria Task Force. J Am Coll Radiol. (2016) 13:e1–29. 10.1016/j.jacr.2015.07.007 - DOI - PubMed
-
- Maisch B, Seferović PM, Ristić AD, Erbel R, Rienmüller R, Adler Y, et al. Guidelines on the diagnosis and management of pericardial diseases executive summary; The Task force on the diagnosis and management of pericardial diseases of the European society of cardiology. Eur Heart J. (2004) 25:587–610. 10.1016/j.ehj.2004.02.002 - DOI - PubMed
-
- Chikuie E, Fugisaki S, Fukuhara S, Imaoka K, Hirata Y, Fukuda S, et al. A rare case oesophageal perforation by a fish bone, leading to pericardial penetration and cardiac tamponade. Hiroshima J Med Sci. (2018) 67:47–9. 10.24811/hjms.67.2_47 - DOI
Publication types
LinkOut - more resources
Full Text Sources
Research Materials