

Myoclonus-Ataxia Syndromes: A Diagnostic Approach
- PMID: 33426154
- PMCID: PMC7780951
- DOI: 10.1002/mdc3.13106
Myoclonus-Ataxia Syndromes: A Diagnostic Approach
Abstract
Background: A myriad of disorders combine myoclonus and ataxia. Most causes are genetic and an increasing number of genes are being associated with myoclonus-ataxia syndromes (MAS), due to recent advances in genetic techniques. A proper etiologic diagnosis of MAS is clinically relevant, given the consequences for genetic counseling, treatment, and prognosis.
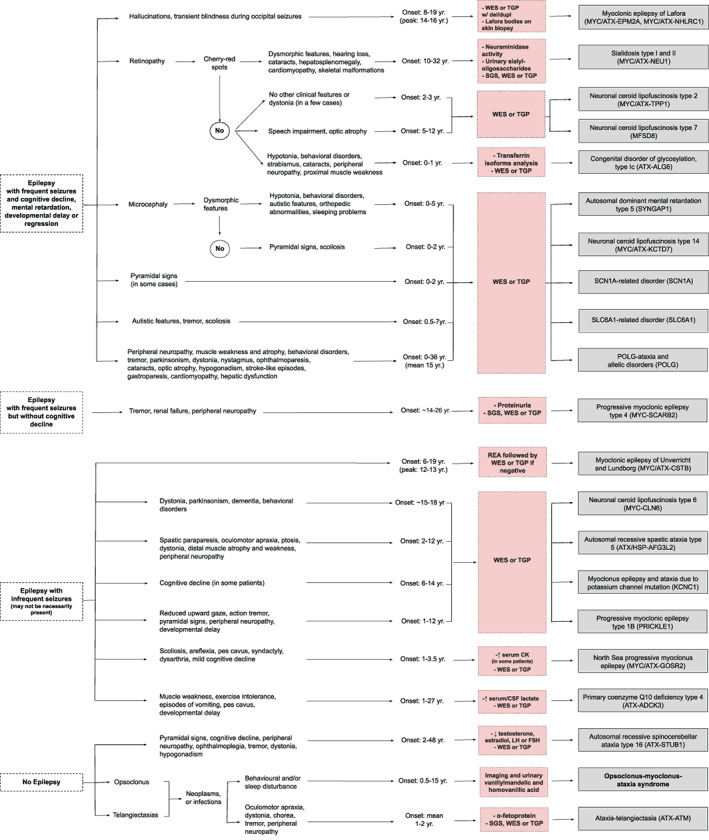
Objectives: To review the causes of MAS and to propose a diagnostic algorithm.
Methods: A comprehensive and structured literature search following PRISMA criteria was conducted to identify those disorders that may combine myoclonus with ataxia.
Results: A total of 135 causes of combined myoclonus and ataxia were identified, of which 30 were charted as the main causes of MAS. These include four acquired entities: opsoclonus-myoclonus-ataxia syndrome, celiac disease, multiple system atrophy, and sporadic prion diseases. The distinction between progressive myoclonus epilepsy and progressive myoclonus ataxia poses one of the main diagnostic dilemmas.
Conclusions: Diagnostic algorithms for pediatric and adult patients, based on clinical manifestations including epilepsy, are proposed to guide the differential diagnosis and corresponding work-up of the most important and frequent causes of MAS. A list of genes associated with MAS to guide genetic testing strategies is provided. Priority should be given to diagnose or exclude acquired or treatable disorders.
Keywords: genetics, myoclonus, ataxia, movement disorders, diagnosis.
© 2020 International Parkinson and Movement Disorder Society.
Conflict of interest statement
This work was generated within the European Reference Network for Rare Neurological Diseases ‐ Project ID No 739510. The authors have no conflicts to report.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
