

Magnetic resonance imaging-derived radiomic signature predicts locoregional failure after organ preservation therapy in patients with hypopharyngeal squamous cell carcinoma
- PMID: 33426314
- PMCID: PMC7780126
- DOI: 10.1016/j.ctro.2020.08.004
Magnetic resonance imaging-derived radiomic signature predicts locoregional failure after organ preservation therapy in patients with hypopharyngeal squamous cell carcinoma
Abstract
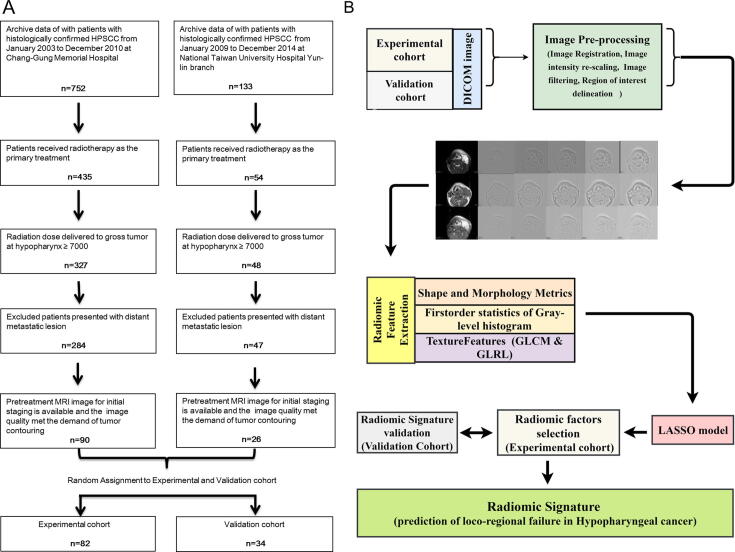
Background and purpose: To develop and validate a magnetic resonance imaging (MRI)-derived radiomic signature (RS) for the prediction of 1-year locoregional failure (LRF) in patients with hypopharyngeal squamous cell carcinoma (HPSCC) who received organ preservation therapy (OPT).
Material and methods: A total of 800 MRI-based features of pretreatment tumors were obtained from 116 patients with HPSCC who received OPT from two independent cohorts. The least absolute shrinkage and selection operator regression model were used to select the features used to develop the RS. Harrell's C-index and corrected C-index were used to evaluate the discriminative ability of RS. The Youden index was used to select the optimal cut-point for risk category.
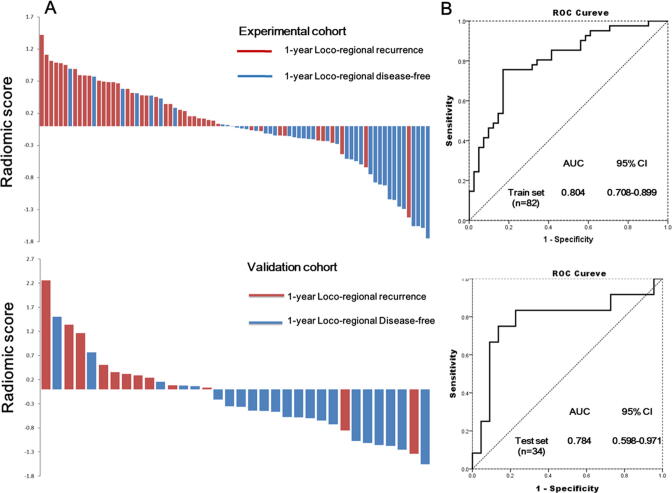
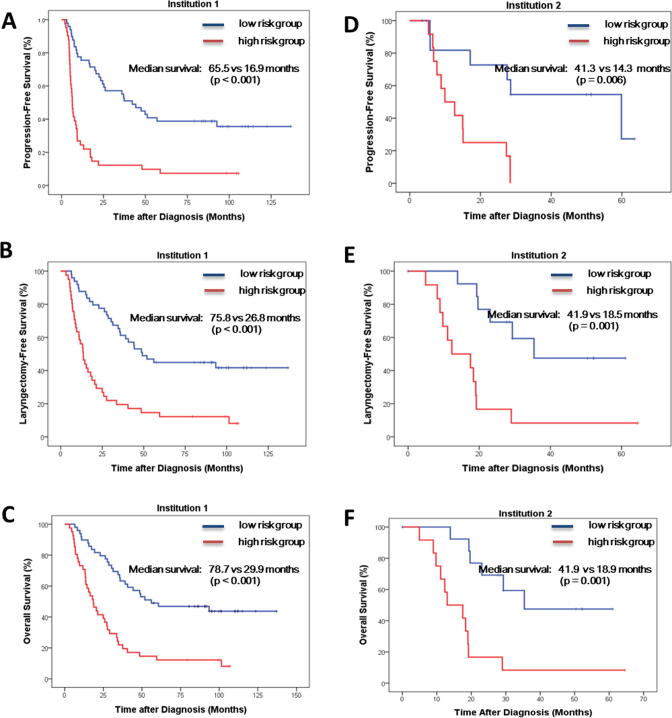
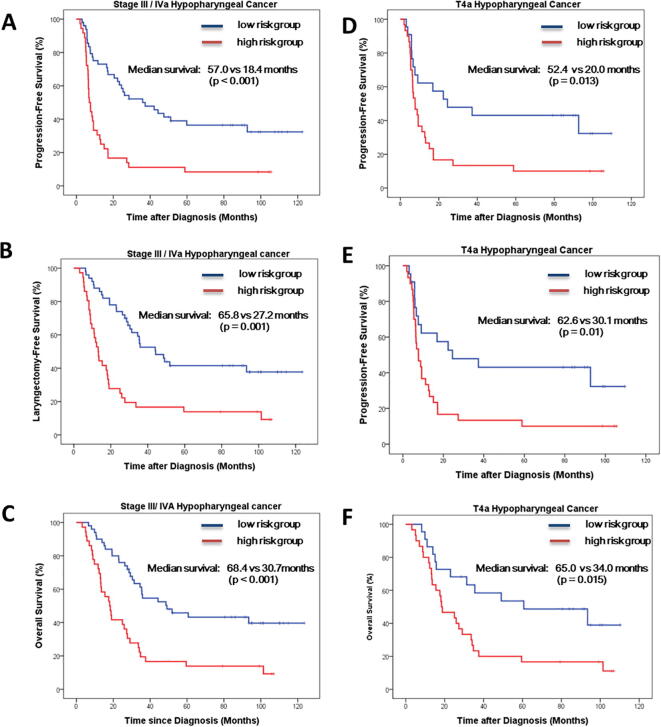
Results: The RS yielded 1000 times bootstrapping corrected C-index of 0.8036 and 0.78235 in the experimental (n = 82) and validation cohorts (n = 34), respectively. With respect to the subgroup of patients with stage III/IV and cT4 disease, the RS also showed good predictive performance with corrected C-indices of 0.760 and 0.754, respectively. The dichotomized risk category using an RS of 0.0326 as the cut-off value yielded a 1-year LRF predictive accuracy of 79.27%, 79.41%, 76.74%, and 71.15% in the experimental, validation, stage III/IV, and cT4a cohorts, respectively. The low-risk group was associated with a significantly better progression-free laryngectomy-free and overall survival outcome in two independent institutions, stage III/IV, and cT4a cohorts.
Conclusion: The RS-based model provides a novel and convenient approach for the prediction of the 1-year LRF and survival outcome in patients with HPSCC who received OPT.
Keywords: Hypopharyngeal squamous cell carcinoma; Loco-regional failure; Organ preservation treatment; Radiomics; Survival.
© 2020 The Author(s).
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Radiomics in Hypopharyngeal Cancer Management: A State-of-the-Art Review.Biomedicines. 2023 Mar 6;11(3):805. doi: 10.3390/biomedicines11030805. Biomedicines. 2023. PMID: 36979783 Free PMC article. Review.
-
Radiomics Nomogram for Predicting Locoregional Failure in Locally Advanced Non-small Cell Lung Cancer Treated with Definitive Chemoradiotherapy.Acad Radiol. 2022 Feb;29 Suppl 2:S53-S61. doi: 10.1016/j.acra.2020.11.018. Epub 2020 Dec 8. Acad Radiol. 2022. PMID: 33308945
-
Prognostic value of the radiomics-based model in progression-free survival of hypopharyngeal cancer treated with chemoradiation.Eur Radiol. 2020 Feb;30(2):833-843. doi: 10.1007/s00330-019-06452-w. Epub 2019 Oct 30. Eur Radiol. 2020. PMID: 31673835
-
Predicting Progression-Free Survival Using MRI-Based Radiomics for Patients With Nonmetastatic Nasopharyngeal Carcinoma.Front Oncol. 2020 May 12;10:618. doi: 10.3389/fonc.2020.00618. eCollection 2020. Front Oncol. 2020. PMID: 32477932 Free PMC article.
-
Magnetic resonance imaging radiomics predicts preoperative axillary lymph node metastasis to support surgical decisions and is associated with tumor microenvironment in invasive breast cancer: A machine learning, multicenter study.EBioMedicine. 2021 Jul;69:103460. doi: 10.1016/j.ebiom.2021.103460. Epub 2021 Jul 4. EBioMedicine. 2021. PMID: 34233259 Free PMC article. Clinical Trial.
Cited by
-
An MRI-based radiomics-clinical nomogram for the overall survival prediction in patients with hypopharyngeal squamous cell carcinoma: a multi-cohort study.Eur Radiol. 2022 Mar;32(3):1548-1557. doi: 10.1007/s00330-021-08292-z. Epub 2021 Oct 19. Eur Radiol. 2022. PMID: 34665315
-
Radiomics in Hypopharyngeal Cancer Management: A State-of-the-Art Review.Biomedicines. 2023 Mar 6;11(3):805. doi: 10.3390/biomedicines11030805. Biomedicines. 2023. PMID: 36979783 Free PMC article. Review.
-
Exploratory ensemble interpretable model for predicting local failure in head and neck cancer: the additive benefit of CT and intra-treatment cone-beam computed tomography features.Quant Imaging Med Surg. 2021 Dec;11(12):4781-4796. doi: 10.21037/qims-21-274. Quant Imaging Med Surg. 2021. PMID: 34888189 Free PMC article.
-
Intensity standardization methods in magnetic resonance imaging of head and neck cancer.Phys Imaging Radiat Oncol. 2021 Nov 20;20:88-93. doi: 10.1016/j.phro.2021.11.001. eCollection 2021 Oct. Phys Imaging Radiat Oncol. 2021. PMID: 34849414 Free PMC article.
-
An MRI-based radiomics nomogram for detecting cervical esophagus invasion in hypopharyngeal squamous cell carcinoma.Cancer Imaging. 2023 Dec 15;23(1):120. doi: 10.1186/s40644-023-00642-y. Cancer Imaging. 2023. PMID: 38102719 Free PMC article.
References
-
- Jemal A., Bray F., Center M.M., Ferlay J., Ward E., Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. - PubMed
-
- Carvalho A.L., Nishimoto I.N., Califano J.A., Kowalski L.P. Trends in incidence and prognosis for head and neck cancer in the United States: a site-specific analysis of the SEER database. Int J Cancer. 2005;114:806–816. - PubMed
-
- Lee N.Y., O’Meara W., Chan K. Concurrent chemotherapy and intensity-modulated radiotherapy for locoregionally advanced laryngeal and hypopharyngeal cancers. Int J Radiat Oncol Biol Phys. 2007;69:459–468. - PubMed
LinkOut - more resources
Full Text Sources
