

Mechanisms, features, and significance of diastolic mitral regurgitation: a case series
- PMID: 33426438
- PMCID: PMC7780436
- DOI: 10.1093/ehjcr/ytaa203
Mechanisms, features, and significance of diastolic mitral regurgitation: a case series
Abstract
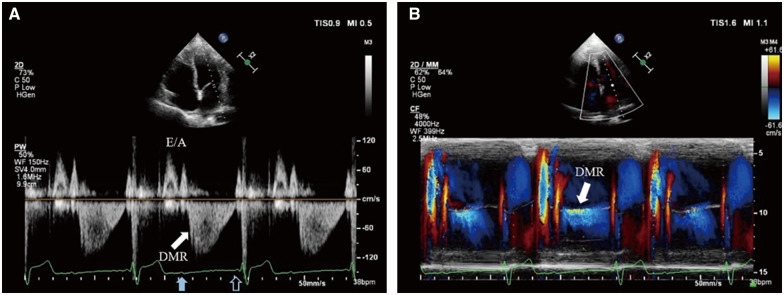
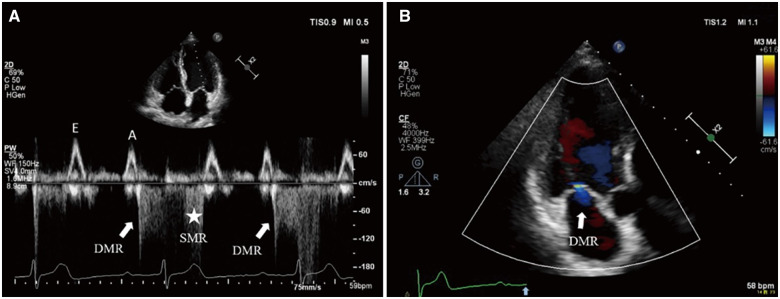
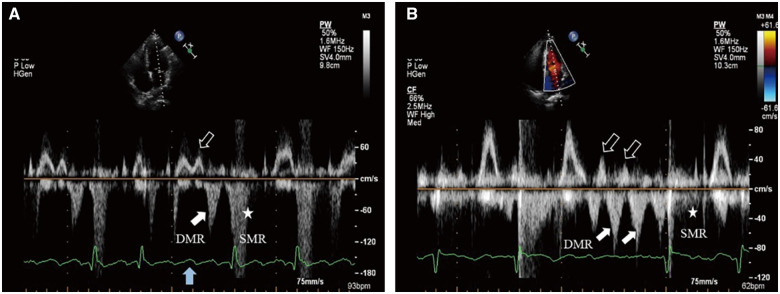
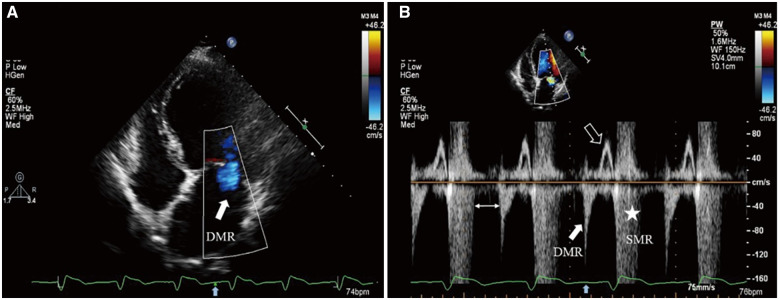
Background: Diastolic mitral regurgitation (DMR) is a type of functional mitral regurgitation. Its occurrence in the diastolic phase of cardiac cycle renders DMR an easily ignored entity. Confusing it with systolic mitral regurgitation occasionally happens. The reversal of left atrioventricular pressure gradient during diastole and the incomplete closure of mitral valve are the essential conditions for DMR. Diastolic mitral regurgitation develops under various situations, where the mechanisms of diastolic reversal of left atrioventricular pressure gradient differ.
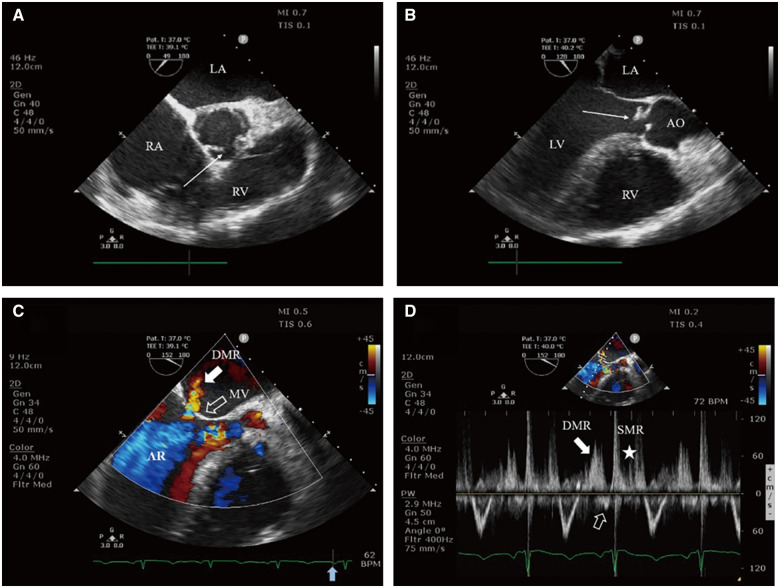
Case summary: Patient 1 was a 50-year-old man diagnosed with 2:1 second-degree atrioventricular block (AVB). Patient 2 was a 70-year-old man diagnosed with first-degree AVB. Patient 3 was a 66-year-old man diagnosed with atrial fibrillation with long intermission and occasional atrial flutter with unequal conduction. Patient 4 was a 54-year-old woman diagnosed with dilated cardiomyopathy with complete left bundle branch block. Patient 5 was a 36-year-old man diagnosed with severe acute aortic regurgitation secondary to subacute bacterial endocarditis.
Discussion: Although the degree of DMR is relatively mild, its appearance generally prompts further clinical considerations. The appreciation of DMR has an incremental value for diagnosing and evaluating the underlying cardiovascular disease.
Keywords: Case series; Diastolic mitral regurgitation; Functional mitral regurgitation; Mechanisms.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Similar articles
-
Different mechanisms for diastolic mitral regurgitation illustrated by three comparative cases.Echocardiography. 2011 Apr;28(4):476-9. doi: 10.1111/j.1540-8175.2010.01323.x. Epub 2011 Mar 14. Echocardiography. 2011. PMID: 21395668
-
Diastolic Mitral Regurgitation With Interatrial Left-to-Right Shunt.JACC Case Rep. 2025 Mar 19;30(6 Pt 2):103417. doi: 10.1016/j.jaccas.2025.103417. JACC Case Rep. 2025. PMID: 40155120 Free PMC article.
-
Diastolic mitral regurgitation following transcatheter aortic valve replacement: Incidence, predictors, and association with clinical outcomes.J Cardiol. 2017 Nov;70(5):491-497. doi: 10.1016/j.jjcc.2017.01.007. Epub 2017 Apr 1. J Cardiol. 2017. PMID: 28377025
-
Complete atrioventricular block with diastolic mitral regurgitation due to severe lithium intoxication. A case report.Acta Cardiol. 2022 Dec;77(10):873-878. doi: 10.1080/00015385.2022.2054493. Epub 2022 Mar 24. Acta Cardiol. 2022. PMID: 35322750 Review.
-
Restoration of normal left ventricular geometry after percutaneous mitral annuloplasty: case report and review of literature.Catheter Cardiovasc Interv. 2015 Aug;86(2):E107-10. doi: 10.1002/ccd.25689. Epub 2014 Oct 7. Catheter Cardiovasc Interv. 2015. PMID: 25258184 Review.
Cited by
-
Diastolic Mitral Regurgitation as a Rare Cause of Acute Respiratory Failure Following Complete Atrioventricular Block.JACC Case Rep. 2023 Jul 25;21:101961. doi: 10.1016/j.jaccas.2023.101961. eCollection 2023 Sep 6. JACC Case Rep. 2023. PMID: 37719296 Free PMC article.
-
Left ventricular haemodynamic effects in a patient with endocarditis.Neth Heart J. 2021 Dec;29(12):668-669. doi: 10.1007/s12471-021-01616-0. Epub 2021 Aug 17. Neth Heart J. 2021. PMID: 34403068 Free PMC article. No abstract available.
-
Heart rate-dependent mitral regurgitation.Clin Case Rep. 2023 Oct 3;11(10):e8003. doi: 10.1002/ccr3.8003. eCollection 2023 Oct. Clin Case Rep. 2023. PMID: 37799565 Free PMC article.
-
A Reverse Mitral A-Wave and a Late Systolic Tricuspid Regurgitation Jet due to Retrograde Atrial Activation.CASE (Phila). 2024 May 7;8(6):364-368. doi: 10.1016/j.case.2024.04.002. eCollection 2024 Jun. CASE (Phila). 2024. PMID: 38983645 Free PMC article.
References
-
- Enriquez-Sarano M, Akins CW, Vahanian A.. Mitral regurgitation. Lancet 2009;373:1382–1394. - PubMed
-
- Sisu RC, Vinereanu D.. Different mechanisms for diastolic mitral regurgitation illustrated by three comparative cases. Echocardiography 2011;28:476–479. - PubMed
-
- Agricola E, Galderisi M, Mele D, Ansalone G, Dini FL, Di Salvo G,. et al. Echocardiographic Study Group of the Italian Society of C. Mechanical dyssynchrony and functional mitral regurgitation: pathophysiology and clinical implications. J Cardiovasc Med (Hagerstown) 2008;9:461–469. - PubMed
-
- Nof E, Glikson M, Bar-Lev D, Gurevitz O, Luria D, Eldar M. et al. Mechanism of diastolic mitral regurgitation in candidates for cardiac resynchronization therapy. Am J Cardiol 2006;97:1611–1614. - PubMed
LinkOut - more resources
Full Text Sources