

IGF-Binding Proteins, Adiponectin, and Survival in Metastatic Colorectal Cancer: Results From CALGB (Alliance)/SWOG 80405
- PMID: 33426464
- PMCID: PMC7785047
- DOI: 10.1093/jncics/pkaa074
IGF-Binding Proteins, Adiponectin, and Survival in Metastatic Colorectal Cancer: Results From CALGB (Alliance)/SWOG 80405
Abstract
Background: Energy balance-related biomarkers are associated with risk and prognosis of various malignancies. Their relationship to survival in metastatic colorectal cancer (mCRC) requires further study.
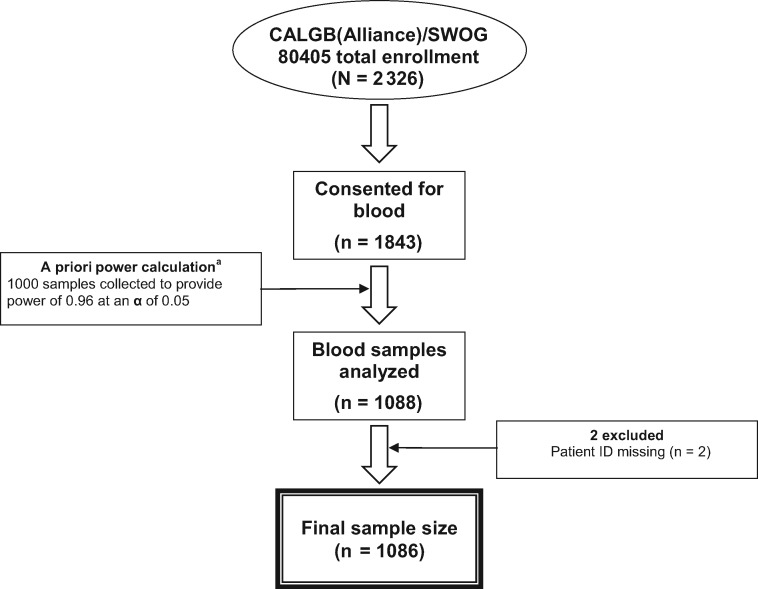
Methods: Baseline plasma insulin-like growth factor (IGF)-1, IGF-binding protein (IGFBP)-3, IGFBP-7, C-peptide, and adiponectin were measured at time of trial registration in a prospective cohort of patients with mCRC participating in a National Cancer Institute-sponsored trial of first-line systemic therapy. We used Cox proportional hazards regression to adjust for confounders and examine associations of each biomarker with overall survival (OS) and progression-free survival (PFS). P values are 2-sided.
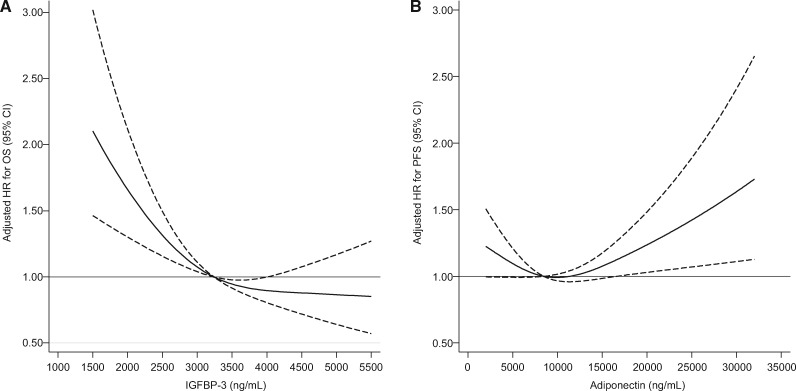
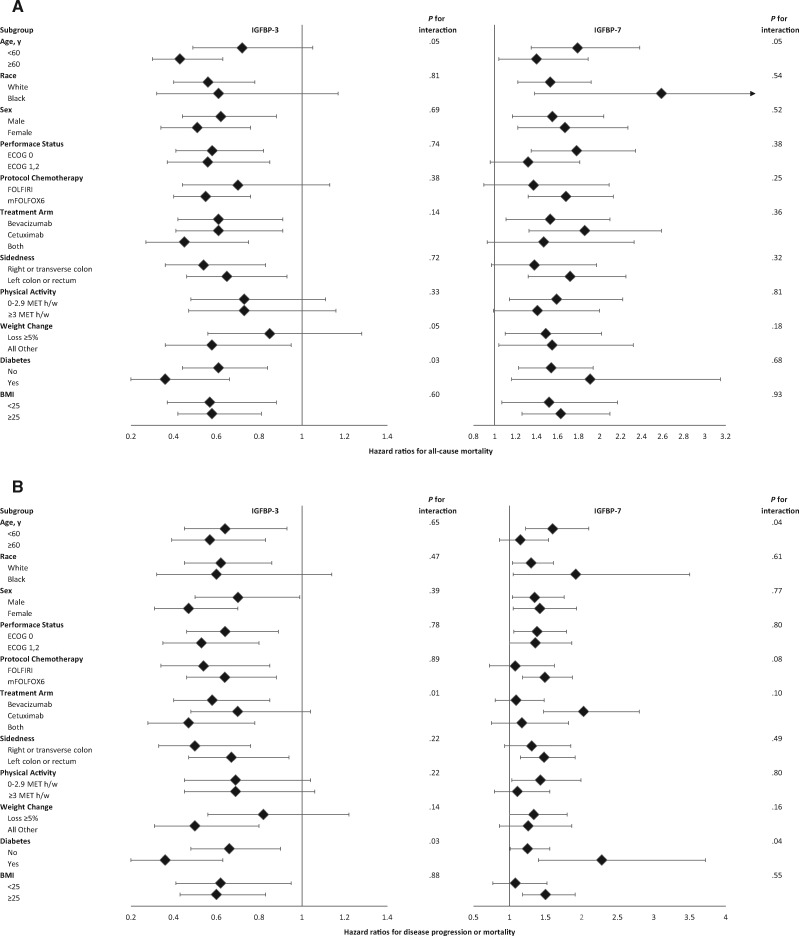
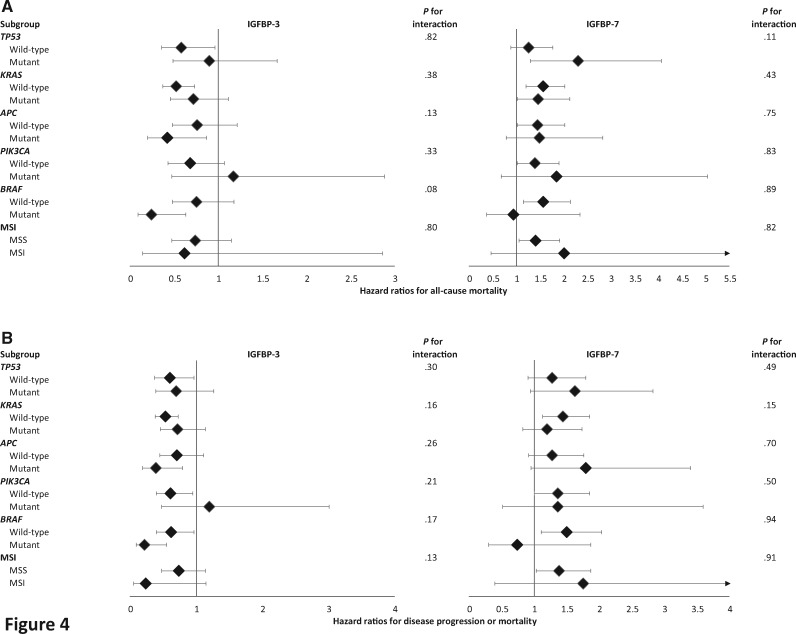
Results: Median follow-up for 1086 patients was 6.2 years. Compared with patients in the lowest IGFBP-3 quintile, patients in the highest IGFBP-3 quintile experienced an adjusted hazard ratio (HR) for OS of 0.57 (95% confidence interval [CI] = 0.42 to 0.78; P nonlinearity < .001) and for PFS of 0.61 (95% CI = 0.45 to 0.82; P trend = .003). Compared with patients in the lowest IGFBP-7 quintile, patients in the highest IGFBP-7 quintile experienced an adjusted hazard ratio for OS of 1.60 (95% CI = 1.30 to 1.97; P trend < .001) and for PFS of 1.38 (95% CI = 1.13 to 1.69; P trend < .001). Plasma C-peptide and IGF-1 were not associated with patient outcomes. Adiponectin was not associated with OS; there was a nonlinear U-shaped association between adiponectin and PFS (P nonlinearity = .03).
Conclusions: Among patients with mCRC, high plasma IGFBP-3 and low IGFBP-7 were associated with longer OS and PFS. Extreme levels of adiponectin were associated with shorter PFS. These findings suggest potential avenues for prognostic and therapeutic innovation.
© The Author(s) 2020. Published by Oxford University Press.
Figures
References
-
- Howlader N, Noone AM, Krapcho M, et al. SEER Cancer Statistics Review, 1975-2017. Bethesda, MD: National Cancer Institute; 2020.
-
- Pollak M. The insulin and insulin-like growth factor receptor family in neoplasia: an update. Nat Rev Cancer. 2012;12(3):159-169. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U10 CA180826/CA/NCI NIH HHS/United States
- R01 CA118553/CA/NCI NIH HHS/United States
- R01 CA149222/CA/NCI NIH HHS/United States
- U10 CA180821/CA/NCI NIH HHS/United States
- R00 CA218603/CA/NCI NIH HHS/United States
- U10 CA180795/CA/NCI NIH HHS/United States
- P30 CA008748/CA/NCI NIH HHS/United States
- UG1 CA233373/CA/NCI NIH HHS/United States
- U10 CA180882/CA/NCI NIH HHS/United States
- U10 CA180820/CA/NCI NIH HHS/United States
- U10 CA180888/CA/NCI NIH HHS/United States
- U10 CA180830/CA/NCI NIH HHS/United States
- U10 CA180836/CA/NCI NIH HHS/United States
- UG1 CA189858/CA/NCI NIH HHS/United States
- U10 CA180790/CA/NCI NIH HHS/United States
- R01 CA169141/CA/NCI NIH HHS/United States
- UG1 CA233180/CA/NCI NIH HHS/United States
- U10 CA180867/CA/NCI NIH HHS/United States
- U10 CA180838/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous