

Astroglial tau pathology alone preferentially concentrates at sulcal depths in chronic traumatic encephalopathy neuropathologic change
- PMID: 33426528
- PMCID: PMC7784042
- DOI: 10.1093/braincomms/fcaa210
Astroglial tau pathology alone preferentially concentrates at sulcal depths in chronic traumatic encephalopathy neuropathologic change
Abstract
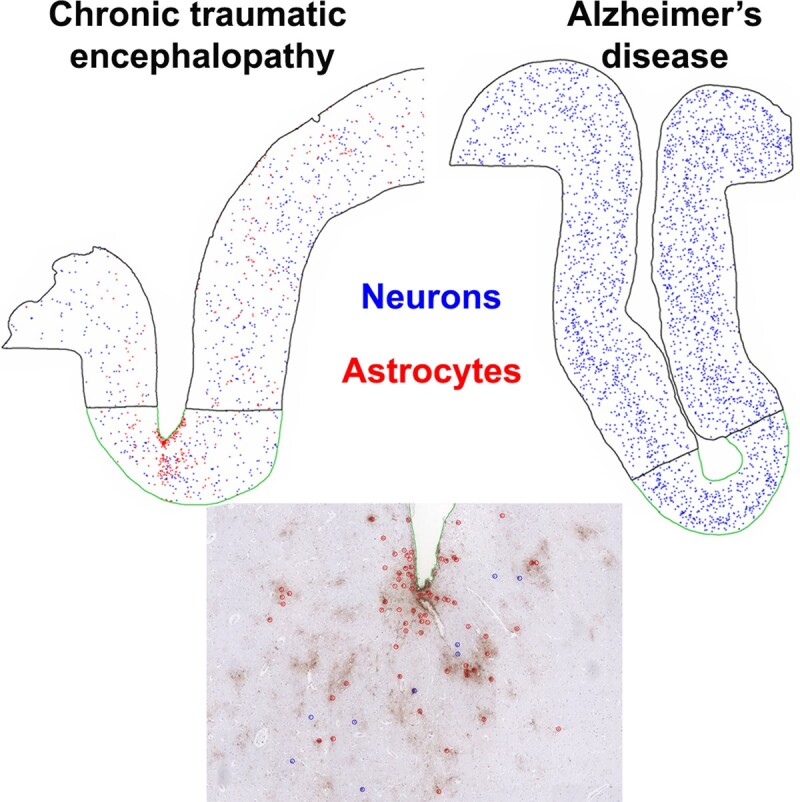
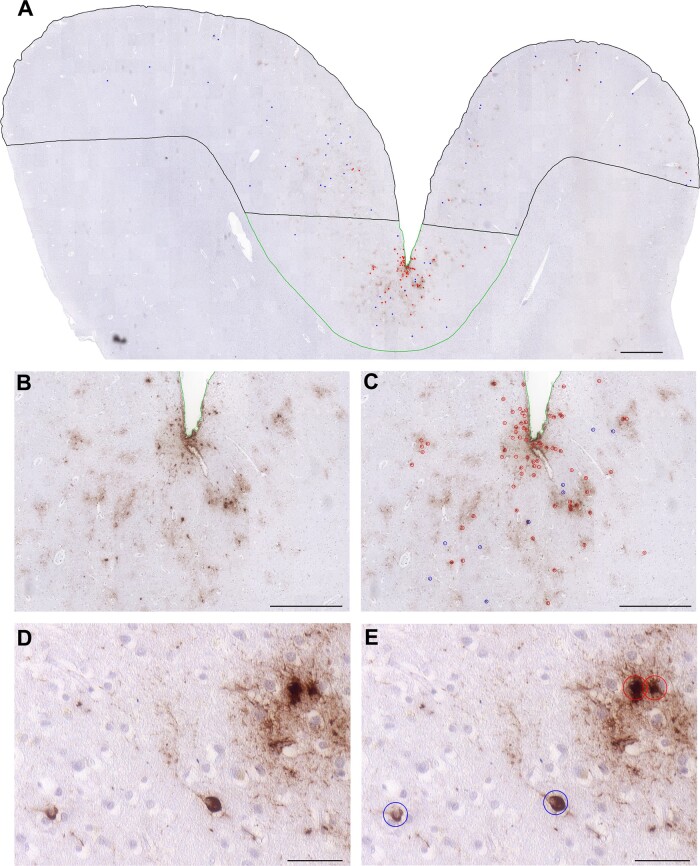
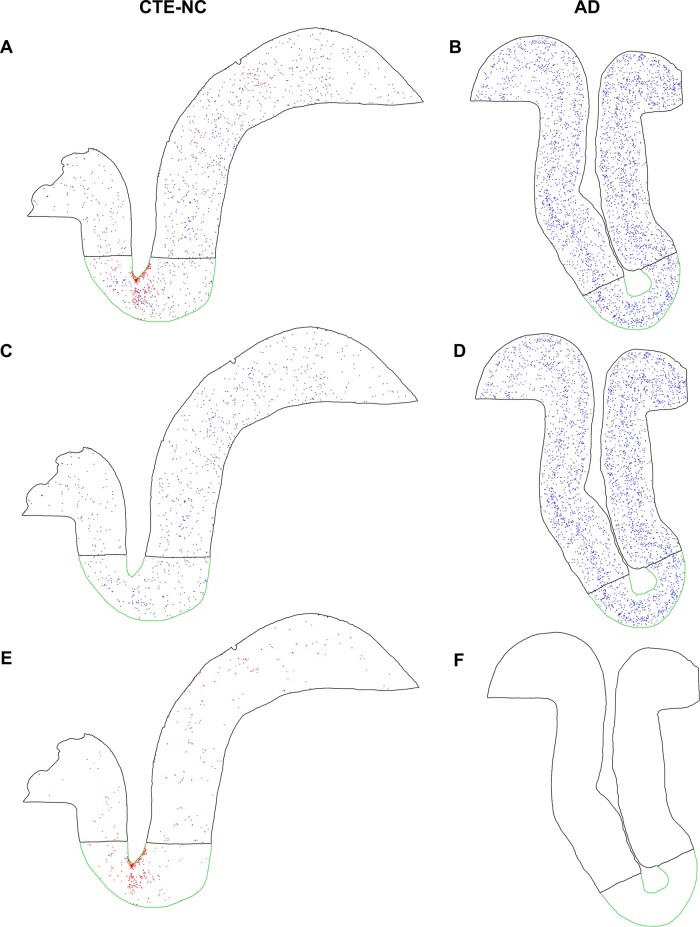
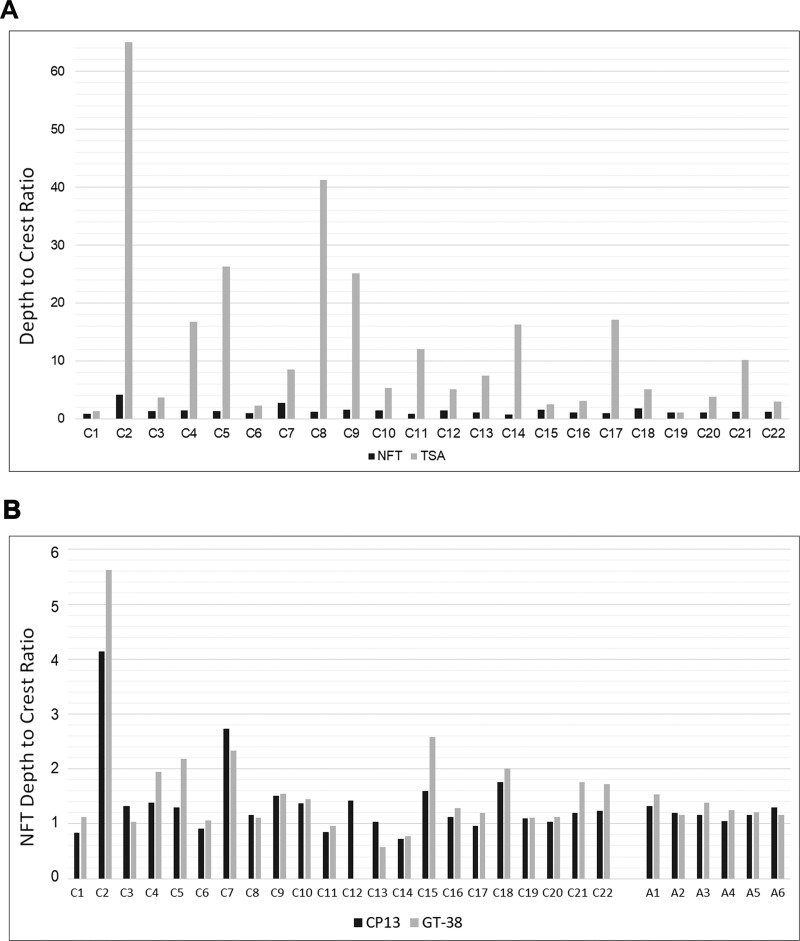
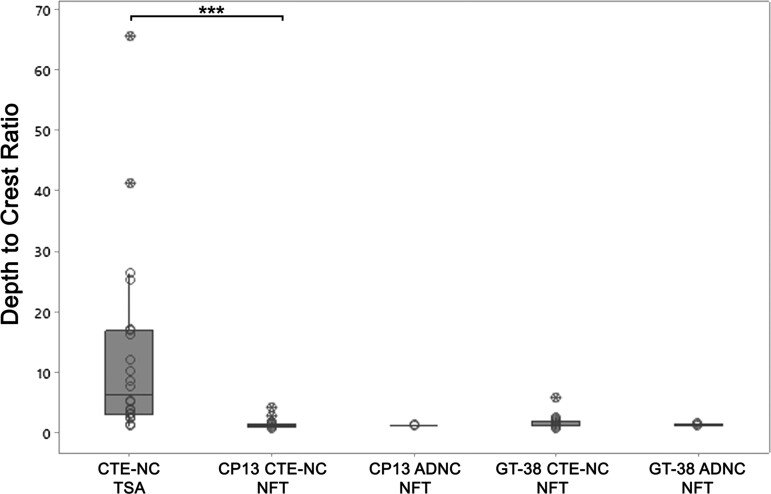
Current diagnostic criteria for the neuropathological evaluation of the traumatic brain injury-associated neurodegeneration, chronic traumatic encephalopathy, define the pathognomonic lesion as hyperphosphorylated tau-immunoreactive neuronal and astroglial profiles in a patchy cortical distribution, clustered around small vessels and showing preferential localization to the depths of sulci. However, despite adoption into diagnostic criteria, there has been no formal assessment of the cortical distribution of the specific cellular components defining chronic traumatic encephalopathy neuropathologic change. To address this, we performed comprehensive mapping of hyperphosphorylated tau-immunoreactive neurofibrillary tangles and thorn-shaped astrocytes contributing to chronic traumatic encephalopathy neuropathologic change. From the Glasgow Traumatic Brain Injury Archive and the University of Pennsylvania Center for Neurodegenerative Disease Research Brain Bank, material was selected from patients with known chronic traumatic encephalopathy neuropathologic change, either following exposure to repetitive mild (athletes n = 17; non-athletes n = 1) or to single moderate or severe traumatic brain injury (n = 4), together with material from patients with previously confirmed Alzheimer's disease neuropathologic changes (n = 6) and no known exposure to traumatic brain injury. Representative sections were stained for hyperphosphorylated or Alzheimer's disease conformation-selective tau, after which stereotypical neurofibrillary tangles and thorn-shaped astrocytes were identified and mapped. Thorn-shaped astrocytes in chronic traumatic encephalopathy neuropathologic change were preferentially distributed towards sulcal depths [sulcal depth to gyral crest ratio of thorn-shaped astrocytes 12.84 ± 15.47 (mean ± standard deviation)], with this pathology more evident in material from patients with a history of survival from non-sport injury than those exposed to sport-associated traumatic brain injury (P = 0.009). In contrast, neurofibrillary tangles in chronic traumatic encephalopathy neuropathologic change showed a more uniform distribution across the cortex in sections stained for either hyperphosphorylated (sulcal depth to gyral crest ratio of neurofibrillary tangles 1.40 ± 0.74) or Alzheimer's disease conformation tau (sulcal depth to gyral crest ratio 1.64 ± 1.05), which was comparable to that seen in material from patients with known Alzheimer's disease neuropathologic changes (P = 0.82 and P = 0.91, respectively). Our data demonstrate that in chronic traumatic encephalopathy neuropathologic change the astroglial component alone shows preferential distribution to the depths of cortical sulci. In contrast, the neuronal pathology of chronic traumatic encephalopathy neuropathologic change is distributed more uniformly from gyral crest to sulcal depth and echoes that of Alzheimer's disease. These observations provide new insight into the neuropathological features of chronic traumatic encephalopathy that distinguish it from other tau pathologies and suggest that current diagnostic criteria should perhaps be reviewed and refined.
Keywords: Alzheimer’s disease; ageing-related tau astrogliopathy; chronic traumatic encephalopathy; tau; traumatic brain injury.
© The Author(s) (2020). Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures

References
-
- Armstrong RA. Quantitative differences in beta/A4 protein subtypes in the parahippocampal gyrus and frontal cortex in Alzheimer’s disease. Dementia 1994; 5: 1–5. - PubMed
Grants and funding
- P30 AG010124/AG/NIA NIH HHS/United States
- RF1 AG054991/AG/NIA NIH HHS/United States
- R01 NS038104/NS/NINDS NIH HHS/United States
- R01 NS094003/NS/NINDS NIH HHS/United States
- F32 AG053036/AG/NIA NIH HHS/United States
- U54 NS115322/NS/NINDS NIH HHS/United States
- TL1 TR001880/TR/NCATS NIH HHS/United States
- R01 NS092398/NS/NINDS NIH HHS/United States
- G0701018/MRC_/Medical Research Council/United Kingdom
- G1100578/MRC_/Medical Research Council/United Kingdom
- P01 AG009215/AG/NIA NIH HHS/United States
- MR/N004272/1/MRC_/Medical Research Council/United Kingdom
- P01 AG017586/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources