

Assessment of peri-implant tissue dimensions following surgical therapy of advanced ligature-induced peri-implantitis defects
- PMID: 33426617
- PMCID: PMC7797391
- DOI: 10.1186/s40729-020-00282-y
Assessment of peri-implant tissue dimensions following surgical therapy of advanced ligature-induced peri-implantitis defects
Abstract
Background: To evaluate peri-implant tissue dimensions following implantoplasty and/or regenerative therapy of advanced ligature-induced peri-implantitis in dogs.
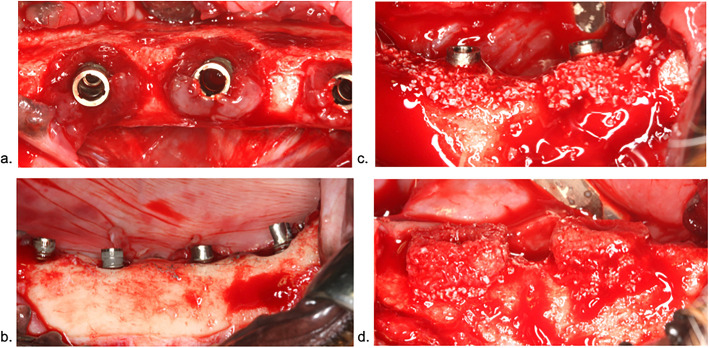
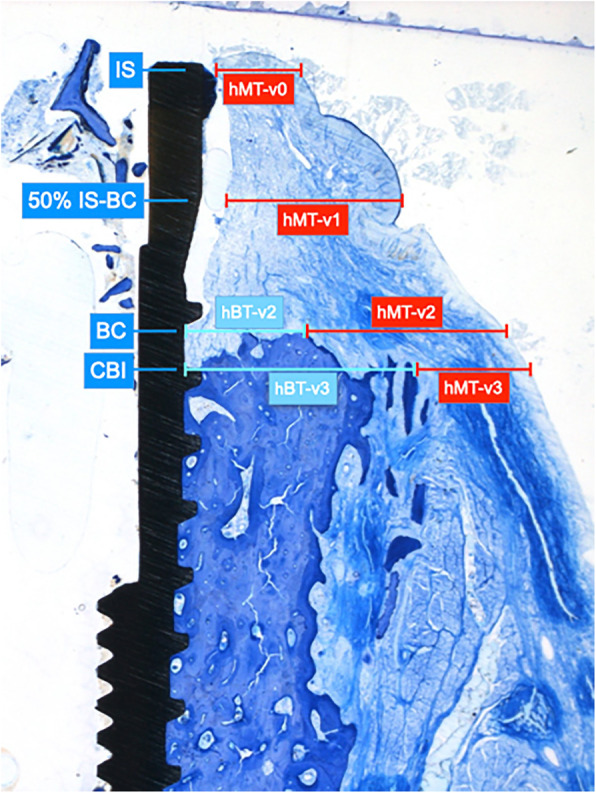
Material and methods: At all defect sites (n = 6 dogs, n = 48 implants), the intrabony component was filled with a particulate bovine-derived natural bone mineral (NBM). The supracrestal component was treated by either the application of an equine bone block (EB) or implantoplasty. In a split-mouth design, NBM and EB were soak-loaded with rhBMP-2 or sterile saline. All sites were covered using a native collagen membrane and left to heal in a submerged position for 12 weeks. The horizontal mucosal thickness (hMT) and bone thickness (hBT) were measured at four reference points: (v0) at the level of implant shoulder (IS), (v1) 50% of the distance IS-bone crest (BC), (v2) at the BC, and (v3) at the most coronal extension of the bone-to-implant contact.
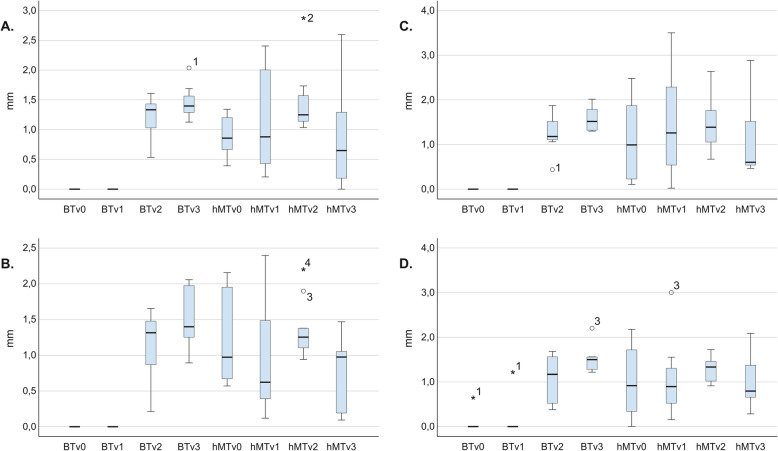
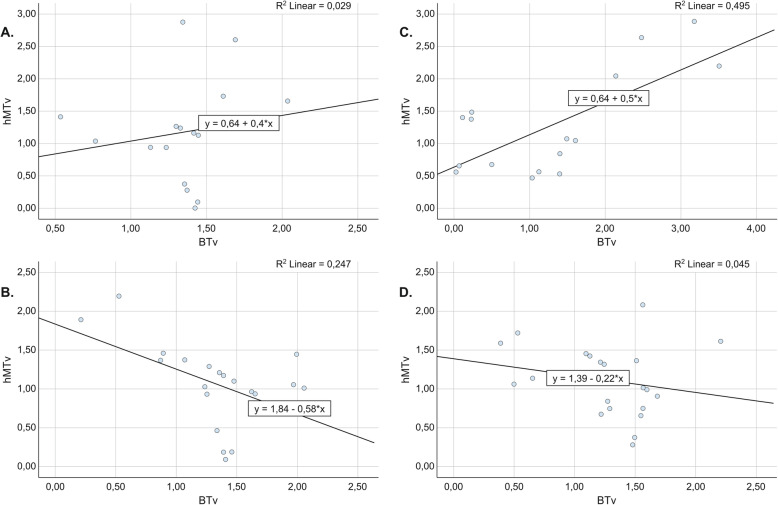
Results: The general tendency indicated a gradual increase in hMT from the IS (v0) toward BC (v2), which was more pronounced at implant sites treated with the regenerative approach. The hBT values increased from v2 to v3, with the highest values at the v3 region measured for implant sites treated with adjunctive rhBMP-2. For sites treated with implantoplasty, the linear regression model demonstrated an inverse correlation between hMT and hBT, whereas a positive correlation was observed at those sites treated with the regenerative approach.
Conclusion: Horizontal soft and hard tissue dimensions were similar among different treatment groups.
Keywords: Animal experiments; Bone regeneration; Dental implant soft tissue; Peri-implantitis treatment.
Conflict of interest statement
The authors Ausra Ramanauskaite, Karina Obreja, Robert Sader, Jürgen Becker, and Frank Schwarz stated explicitly that there are no conflicts of interest related to this article.
Figures
Similar articles
-
Assessment of soft and hard tissue dimensions following different treatment approaches of ligature-induced peri-implantitis defects.Clin Oral Implants Res. 2021 Apr;32(4):394-400. doi: 10.1111/clr.13709. Epub 2021 Jan 27. Clin Oral Implants Res. 2021. PMID: 33421206
-
Surgical therapy of advanced ligature-induced peri-implantitis defects: cone-beam computed tomographic and histological analysis.J Clin Periodontol. 2011 Oct;38(10):939-49. doi: 10.1111/j.1600-051X.2011.01739.x. Epub 2011 Aug 31. J Clin Periodontol. 2011. PMID: 21883358
-
Immunohistochemical characteristics of regenerated bone after surgical therapy of advanced ligature-induced peri-implantitis defects.Clin Oral Investig. 2014 Jul;18(6):1679-86. doi: 10.1007/s00784-013-1138-5. Epub 2013 Nov 24. Clin Oral Investig. 2014. PMID: 24271501
-
Influence of macrophage polarization on the effectiveness of surgical therapy of peri-implantitis.Int J Implant Dent. 2021 Nov 12;7(1):110. doi: 10.1186/s40729-021-00391-2. Int J Implant Dent. 2021. PMID: 34767122 Free PMC article. Review.
-
Experimentally induced peri-implantitis: a review of different treatment methods described in the literature.Int J Oral Maxillofac Implants. 2000 Jul-Aug;15(4):533-44. Int J Oral Maxillofac Implants. 2000. PMID: 10960987 Review.
Cited by
-
Alloplastic Bone Substitutes for Periodontal and Bone Regeneration in Dentistry: Current Status and Prospects.Materials (Basel). 2021 Feb 26;14(5):1096. doi: 10.3390/ma14051096. Materials (Basel). 2021. PMID: 33652888 Free PMC article. Review.
-
Physicochemical and Biological Characterization of Ti6Al4V Particles Obtained by Implantoplasty: An In Vitro Study. Part I.Materials (Basel). 2021 Oct 29;14(21):6507. doi: 10.3390/ma14216507. Materials (Basel). 2021. PMID: 34772034 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
