

Intraoperative imaging technology to maximise extent of resection for glioma: a network meta-analysis
- PMID: 33428222
- PMCID: PMC8094975
- DOI: 10.1002/14651858.CD013630.pub2
Intraoperative imaging technology to maximise extent of resection for glioma: a network meta-analysis
Abstract
Background: Multiple studies have identified the prognostic relevance of extent of resection in the management of glioma. Different intraoperative technologies have emerged in recent years with unknown comparative efficacy in optimising extent of resection. One previous Cochrane Review provided low- to very low-certainty evidence in single trial analyses and synthesis of results was not possible. The role of intraoperative technology in maximising extent of resection remains uncertain. Due to the multiple complementary technologies available, this research question is amenable to a network meta-analysis methodological approach.
Objectives: To establish the comparative effectiveness and risk profile of specific intraoperative imaging technologies using a network meta-analysis and to identify cost analyses and economic evaluations as part of a brief economic commentary.
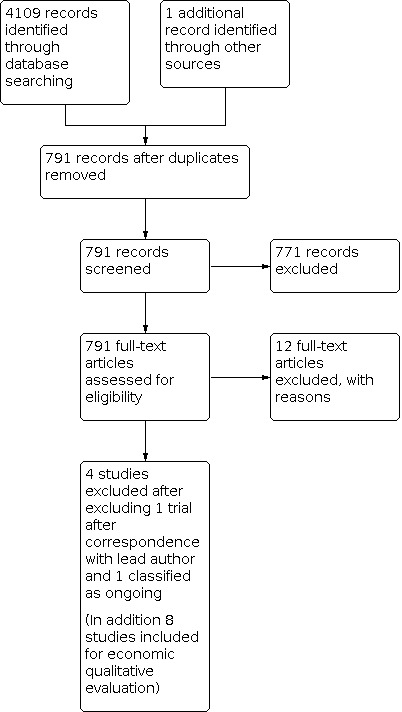
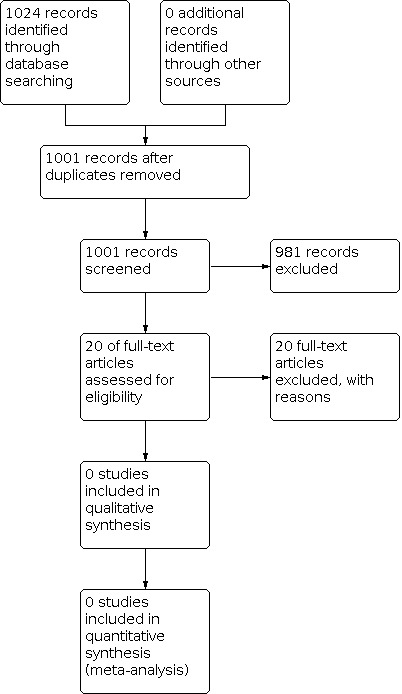
Search methods: We searched CENTRAL (2020, Issue 5), MEDLINE via Ovid to May week 2 2020, and Embase via Ovid to 2020 week 20. We performed backward searching of all identified studies. We handsearched two journals, Neuro-oncology and the Journal of Neuro-oncology from 1990 to 2019 including all conference abstracts. Finally, we contacted recognised experts in neuro-oncology to identify any additional eligible studies and acquire information on ongoing randomised controlled trials (RCTs).
Selection criteria: RCTs evaluating people of all ages with presumed new or recurrent glial tumours (of any location or histology) from clinical examination and imaging (computed tomography (CT) or magnetic resonance imaging (MRI), or both). Additional imaging modalities (e.g. positron emission tomography, magnetic resonance spectroscopy) were not mandatory. Interventions included fluorescence-guided surgery, intraoperative ultrasound, neuronavigation (with or without additional image processing, e.g. tractography), and intraoperative MRI.
Data collection and analysis: Two review authors independently assessed the search results for relevance, undertook critical appraisal according to known guidelines, and extracted data using a prespecified pro forma.
Main results: We identified four RCTs, using different intraoperative imaging technologies: intraoperative magnetic resonance imaging (iMRI) (2 trials, with 58 and 14 participants); fluorescence-guided surgery with 5-aminolevulinic acid (5-ALA) (1 trial, 322 participants); and neuronavigation (1 trial, 45 participants). We identified one ongoing trial assessing iMRI with a planned sample size of 304 participants for which results are expected to be published around winter 2020. We identified no published trials for intraoperative ultrasound. Network meta-analyses or traditional meta-analyses were not appropriate due to absence of homogeneous trials across imaging technologies. Of the included trials, there was notable heterogeneity in tumour location and imaging technologies utilised in control arms. There were significant concerns regarding risk of bias in all the included studies. One trial of iMRI found increased extent of resection (risk ratio (RR) for incomplete resection was 0.13, 95% confidence interval (CI) 0.02 to 0.96; 49 participants; very low-certainty evidence) and one trial of 5-ALA (RR for incomplete resection was 0.55, 95% CI 0.42 to 0.71; 270 participants; low-certainty evidence). The other trial assessing iMRI was stopped early after an unplanned interim analysis including 14 participants; therefore, the trial provided very low-quality evidence. The trial of neuronavigation provided insufficient data to evaluate the effects on extent of resection. Reporting of adverse events was incomplete and suggestive of significant reporting bias (very low-certainty evidence). Overall, the proportion of reported events was low in most trials and, therefore, issues with power to detect differences in outcomes that may or may not have been present. Survival outcomes were not adequately reported, although one trial reported no evidence of improvement in overall survival with 5-ALA (hazard ratio (HR) 0.82, 95% CI 0.62 to 1.07; 270 participants; low-certainty evidence). Data for quality of life were only available for one study and there was significant attrition bias (very low-certainty evidence).
Authors' conclusions: Intraoperative imaging technologies, specifically 5-ALA and iMRI, may be of benefit in maximising extent of resection in participants with high-grade glioma. However, this is based on low- to very low-certainty evidence. Therefore, the short- and long-term neurological effects are uncertain. Effects of image-guided surgery on overall survival, progression-free survival, and quality of life are unclear. Network and traditional meta-analyses were not possible due to the identified high risk of bias, heterogeneity, and small trials included in this review. A brief economic commentary found limited economic evidence for the equivocal use of iMRI compared with conventional surgery. In terms of costs, one non-systematic review of economic studies suggested that, compared with standard surgery, use of image-guided surgery has an uncertain effect on costs and that 5-ALA was more costly. Further research, including completion of ongoing trials of ultrasound-guided surgery, is needed.
Antecedentes: En múltiples estudios se ha identificado la importancia pronóstica del alcance de la resección en el tratamiento del glioma. En los últimos años han surgido diferentes tecnologías intraoperatorias con una eficacia comparativa desconocida para optimizar el alcance de la resección. Una revisión Cochrane anterior proporcionó evidencia de certeza baja a muy baja en los análisis de un solo ensayo y no fue posible la síntesis de los resultados. La función de la tecnología intraoperatoria para maximizar el alcance de la resección aún no está clara. Debido a las múltiples tecnologías complementarias disponibles, esta pregunta de investigación se presta a un enfoque metodológico de metanálisis en red.
Objetivos: Establecer el perfil comparativo de efectividad y riesgo de determinadas tecnologías de imagenología intraoperatorias mediante un metanálisis en red e identificar análisis de costos y evaluaciones económicas como parte de un breve comentario económico. MÉTODOS DE BÚSQUEDA: Se hicieron búsquedas en CENTRAL (2020, número 5), MEDLINE vía Ovid hasta la semana 2 de mayo de 2020, y Embase vía Ovid hasta la semana 20 de 2020. Se realizó una búsqueda retrospectiva de todos los estudios identificados. Se hicieron búsquedas manuales en dos revistas, Neuro‐oncology y Journal of Neuro‐oncology, desde 1990 hasta 2019, y se incluyeron todos los resúmenes de congresos. Finalmente, se estableció contacto con expertos reconocidos en neurooncología para identificar cualquier estudio elegible adicional y obtener información sobre los ensayos controlados aleatorizados (ECA) en curso. CRITERIOS DE SELECCIÓN: ECA que evaluaron a personas de todas las edades con presuntos tumores gliales nuevos o recidivantes (de cualquier ubicación o histología) a partir del examen clínico y la imagenología (tomografía computarizada [TC] o imagenología de resonancia magnética [IRM], o ambas). Las modalidades adicionales de imagenología (p.ej., tomografía de emisión de positrones, espectroscopia de resonancia magnética) no fueron obligatorias. Las intervenciones incluyeron cirugía guiada por fluorescencia, ecografía intraoperatoria, neuronavegación (con o sin procesamiento adicional de las imágenes, p.ej., tractografía) e IRM intraoperatoria. OBTENCIÓN Y ANÁLISIS DE LOS DATOS: Dos autores de la revisión, de forma independiente, evaluaron los resultados de la búsqueda en cuanto a su relevancia, realizaron la evaluación crítica según las guías conocidas y extrajeron los datos mediante un formulario predeterminado.
Resultados principales: Se identificaron cuatro ECA, que utilizaron diferentes tecnologías de imagenología intraoperatorias: la resonancia magnética (IRM) intraoperatoria (dos ensayos, con 58 y 14 participantes); la cirugía guiada por fluorescencia con ácido 5‐aminolevulínico (5‐ALA) (un ensayo, 322 participantes); y la neuronavegación (un ensayo, 45 participantes). Se identificó un ensayo en curso que evaluó la IRM con un tamaño de la muestra planificado de 304 participantes, del que se espera la publicación de los resultados alrededor del invierno de 2020. No se han identificado ensayos publicados sobre la ecografía intraoperatoria. Los metanálisis en red o los metanálisis tradicionales no fueron apropiados debido a la falta de ensayos homogéneos en tecnologías de imagenología. De los ensayos incluidos, hubo una notable heterogeneidad en la localización de los tumores y en las tecnologías de imagenología utilizadas en los brazos control. Hubo inquietudes significativas con respecto al riesgo de sesgo en todos los estudios incluidos. Un ensayo de IRM encontró un aumento en la extensión de la resección (razón de riesgos [RR] para la resección incompleta 0,13; intervalo de confianza [IC] del 95%: 0,02 a 0,96; 49 participantes; evidencia de certeza muy baja) y un ensayo de 5‐ALA (RR para la resección incompleta 0,55; IC del 95%: 0,42 a 0,71; 270 participantes; evidencia de certeza baja). El otro ensayo que evaluó la IRM se interrumpió de forma temprana después de un análisis intermedio no planificado que incluyó 14 participantes; por lo tanto, el ensayo proporciona evidencia de calidad muy baja. El ensayo de neuronavegación no proporcionó datos suficientes para evaluar los efectos sobre el grado de resección. El informe de los eventos adversos fue incompleto e indicó la presencia de sesgo de informe significativo (evidencia de certeza muy baja). En general, la proporción de eventos informados fue baja en la mayoría de los ensayos y, por lo tanto, pueden haber estado presentes o no problemas relacionados con el poder estadístico suficiente para detectar diferencias en los desenlaces. No se informó adecuadamente sobre los desenlaces de supervivencia, aunque un ensayo no informó evidencia de mejora en la supervivencia general con 5‐ALA (cociente de riesgos instantáneos [CRI] 0,82; IC del 95%: 0,62 a 1,07; 270 participantes; evidencia de certeza baja). Solo hubo datos disponibles sobre la calidad de vida de un estudio, con un sesgo de desgaste significativo (evidencia de certeza muy baja).
Conclusiones de los autores: Las tecnologías de imagenología intraoperatoria, específicamente la IRM y el 5‐ALA, pueden ser beneficiosas para maximizar el grado de resección en los participantes con glioma de grado alto. Sin embargo, lo anterior se basa en evidencia de certeza baja a muy baja. Por lo tanto, los efectos neurológicos a corto y a largo plazo no están claros. No están claros los efectos de la cirugía guiada por imágenes sobre la supervivencia general, la supervivencia sin progresión ni la calidad de vida. No fue posible realizar metanálisis en red ni tradicionales debido al alto riesgo de sesgo identificado, a la heterogeneidad y a los ensayos pequeños incluidos en esta revisión. Un comentario económico breve encontró evidencia económica limitada sobre el uso equívoco de la IRM en comparación con la cirugía convencional. En cuanto a los costos, una revisión no sistemática de estudios económicos indicó que, en comparación con la cirugía estándar, el uso de la cirugía guiada por imágenes no tiene un efecto claro sobre los costos y que el ácido 5‐aminolevulínico fue más costoso. Se necesitan estudios de investigación adicionales, incluida la finalización de los ensayos en curso sobre la cirugía guiada por ecografía.
Trial registration: ClinicalTrials.gov NCT01479686.
Copyright © 2021 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Conflict of interest statement
DMF: funded with an NIHR Academic Clinical Fellowship and recipient of a Cancer Research UK Predoctoral Bursary AB: None known DGB: None known MW: None known MGH: None known HB: None known AK: None known CW: None known MDJ: None known
Figures


Update of
- doi: 10.1002/14651858.CD013630
References
References to studies included in this review
Kubben 2014 {published data only (unpublished sought but not used)}
Senft 2011 {published data only (unpublished sought but not used)}
-
- Gessler F, Baumgarten B, Harter P, Baehr O, Franz K, Forster M, Bink A, Seifert V, Senft C. SURG-08. RESECTION OF CONTRAST ENHANCING TISSUE PROLONGS OVERALL SURVIVAL IN GLIOMAS – SECONDARY ENDPOINT ANALYSIS OF A RANDOMIZED CONTROLLED TRIAL ON INTRAOPERATIVE MRI USE. Neuro-Oncology November 2017;19(suppl_6):vi237.
-
- Senft C, Bink A, Franz K, Gasser T, Seifert V. Intra-operative MRI-guided vs. conventional microsurgical brain tumor resection - results of a prospective randomized trial. Journal of Neurosurgery 2011;115:Abstract 602.
-
- Senft C, Bink A, Franz K, Vatter H, Gasser T, Seifert V. Intraoperative MRI guidance and extent of resection in glioma surgery: a randomised, controlled trial. Lancet Oncology 2011;12(11):997-1003. - PubMed
-
- Senft C, Bink A, Heckelmann M, Gasser T, Seifert V. Glioma extent of resection and ultra-low-field iMRI: interim analysis of a prospective randomized controlled trial. Acta Neurochirurgica Supplementum 2011;109:49-53. - PubMed
Stummer 2006 {published data only}
-
- Stummer W, Pichlmeier U, Meinel T, Wiestler OD, Zanella F, Roulen HJ, ALA Glioma Study Group. Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: a randomised controlled multicentre phase III trial. Lancet Oncology 2006;7(5):392-401. - PubMed
-
- Stummer W, Reulen HJ, Meinel T, Pichelmeier U, Schumacher W, Tonn JC, et al, ALA Glioma Study Group. Extent of resection and survival in glioblastoma multiforme: identification of and adjustment for bias. Neurosurgery 2008;62:564-76. - PubMed
-
- Stummer W, Tonn JC, Mehdorn HM, Nestler U, Franz K, Goetz C, et al, ALA-Glioma Study group. Counterbalancing risks and gains from extended resections in malignant glioma surgery: a supplemental analysis from the randomized 5-aminolevulinic acid glioma resection study. Journal of Neurosurgery 2011;114(3):613-23. - PubMed
Willems 2006 {published data only}
-
- Willems PW, Taphoorn MJ, Burger H, Berkelbach van der Sprenkel JW, Tulleken CA. Effectiveness of neuronavigation in resecting solitary intracerebral contrast-enhancing tumors: a randomized controlled trial. Journal of Neurosurgery 2006;104(3):360-8. - PubMed
References to studies excluded from this review
Abraham 2018 {published data only}
-
- Abraham P, Sarkar R, Brandel M, Wali A, Rennert R, Ramos CL, et al. Cost-effectiveness of intraoperative MRI in the treatment of high-grade gliomas. Neuro-oncology 2018;20(Suppl 6):vi146.
Abraham 2019 {published data only}
Chen 2011 {published data only}
-
- Chen X, Meng X, Zhang J, Wang F, Zhao Y, Xu BN. Low- grade insular glioma resection with 1.5T intra-operative MRI: preliminary results of a prospective randomized trial. Neuro-oncology 2011;13(iii):57.
Chen 2012 {published data only (unpublished sought but not used)}
-
- Chen X, Meng X, Zhang J, Li F, Li J, Xu BN. Low- grade insular glioma resection with 1.5t intra-operative MRI: preliminary results of a prospective randomized trial. Journal of Neurosurgery 2012;117(2):A406–7.
Czyz 2011 {published data only}
-
- Czyz M, Tabakow P, Lechowicz-Glogowska B, Jarmundowicz W. Prospective study on the efficacy of low-field intraoperative magnetic resonance imaging in neurosurgical operations. Neurologia i Neurochirurgia Polska 2011;45(3):226-34. - PubMed
Eljamel 2008 {published data only}
-
- Eljamel MS, Goodman C, Moseley H. ALA and Photofrin fluorescence-guided resection and repetitive PDT in glioblastoma multiforme: a single centre phase III randomised controlled trial. Lasers in Medical Science 2008;23(4):361-7. - PubMed
Golub 2020 {published data only}
-
- Golub D, Hyde J, Dogra S, Nicholson J, Kirkwood KA, Gohel P, et al. Intraoperative MRI versus 5-ALA in high-grade glioma resection: a network meta-analysis. Journal of Neurosurgery 2020 Feb;21:1-15. - PubMed
Koc 2008 {published data only}
-
- Koc K. Fluorescein sodium-guided surgery in glioblastoma multiforme: a prospective evaluation. British Journal of Neurosurgery 2008;22(1):99-103. - PubMed
Rohde 2011 {published data only}
-
- Rohde V, Coenen VA. Intraoperative 3-dimensional ultrasound for resection control during brain tumour removal: preliminary results of a prospective randomized study. Acta Neuropathologica 2011;109(Supplementum):187-90. - PubMed
Seddighi 2016 {published data only (unpublished sought but not used)}
-
- Seddighi A, Seddighi AS, Nikouei A, Mohseni G. Image guided surgery using neuronavigation system in resection of cerebral gliomas involving eloquent cortical areas in pediatric population. Neuro-oncology 2016;18(iii):128.
Stepp 2007 {published data only}
-
- Stepp H, Beck T, Pongratz T, Meinel T, Kreth FW, Tonn JCh, et al. ALA and malignant glioma: fluorescence- guided resection and photodynamic treatment. Journal of Environmental Pathology, Toxicology and Oncology 2007;26(2):157-64. - PubMed
Stummer 2017 {published data only}
Wadhwa 2019 {published data only}
-
- Wadhwa S, Malhotra M, Walia B, Kumar A, Aggarwal B. Role of Intraoperative MRI (iMRI) in neurosurgery, potential imaging tool for maximizing gross total resection (GTR) rate of CNS tumours. Annals of Oncology 2019;30(Suppl 5):v156-7.
Waqas 2018 {published data only}
-
- Waqas M, Shamim MS. Sodium fluorescein guided resection of malignant glioma. Journal of the Pakistan Medical Association 2018;68(6):968-70. - PubMed
Wu 2003 {published data only (unpublished sought but not used)}
-
- Wu JS, Zhou LF, Hong XN, Mao Y, Du GH. Role of diffusion tensor imaging in neuronavigation surgery of brain tumors involving pyramidal tracts. Zhonghua Wai Ke za Zhi [Chinese Journal of Surgery] 2003;41(9):662-6. - PubMed
Wu 2004 {published data only (unpublished sought but not used)}
-
- Wu JS, Zhou LF, Gao GJ, Mao Y, Du GH. Integrating functional magnetic resonance imaging in neuronavigation surgery of brain tumors involving motor corte. Chinese Medical Journal 2004;84(8):632-6. - PubMed
Wu 2007 {published data only}
-
- Wu JS, Mao Y, Zhou LF, Tang WJ, Hu J, Song YY, et al. Clinical evaluation and follow-up outcome of diffusion tensor imaging-based functional neuronavigation: a prospective, controlled study in patients with gliomas involving pyramidal tracts. Neurosurgery 2007;61(5):935-9. - PubMed
Zhang 2015 {published data only}
-
- Zhang J, Chen X, Zhao Y, Wang F, Li F, Xu B. Impact of intraoperative magnetic resonance imaging and functional neuronavigation on surgical outcome in patients with gliomas involving language areas. Neurosurgical Review 2015;38(2):319-30. - PubMed
References to ongoing studies
NCT00752323 {published data only}
-
- Imaging procedure using ALA in finding residual tumor in grade IV malignant astrocytoma. Ongoing study. August 2008. Contact author for more information.
NCT00977327 {published data only}
-
- Comparison of neuronavigational systems for resection-control of brain tumors. Ongoing study. 2009. Contact author for more information.
NCT01479686 {published data only (unpublished sought but not used)}
-
- Gong X, Yao CJ, Yuan SW, Zhuang DX, Qiu TM, Lu JF, et al. 3.0T iMRI-guided resection of eloquent high-grade gliomas: preliminary results of a randomised controlled trial. Lancet 2015;386:S11.
-
- Wu JS, Gong X, Song YY, Zhuang DX, Yao CJ, Qiu TM, et al. 3.0-T intraoperative magnetic resonance imaging-guided resection in cerebral glioma surgery: interim analysis of a prospective, randomized, triple-blind, parallel-controlled trial. Neurosurgery 2014;61(Suppl 1):145-54. - PubMed
-
- Wu JS, Gong X, Song YY, Zhuang DX, Yao CJ, Qiu TM, et al. 3.0T iMRI guided resection in cerebral glioma surgery: interim analysis of a prospective, randomized, triple-blind, parallel- controlled trial. Clinical Neurosurgery 2013;60:167. - PubMed
NCT01502280 (BALANCE) {published data only}
-
- Fluorescence-guided surgery for low- and high-grade gliomas. Ongoing study. November 2010. Contact author for more information.
NCT01798771 (IMAGER) {published data only}
-
- Intraoperative MRI and 5-ALA guidance to improve the extent of resection in brain tumor surgery (IMAGER). Ongoing study. February 2013. Contact author for more information.
NCT01811121 (RESECT) {published data only}
-
- Medico-economic evaluation of surgery guided by fluorescence for the optimization of resection of glioblastomas (RESECT). Ongoing study. February 2013. Contact author for more information.
NCT02150564 {published and unpublished data}
-
- 3D Ultra Sound for Resection of Brain Tumors (Sono RCT). Ongoing study. October 2016. Contact author for more information.
NCT03291977 (FLEGME) {published data only}
-
- Interest of fluorescein in fluorescence-guided resection of gliomas (FLEGME). Ongoing study. September 2017. Contact author for more information.
NCT03531333 {published data only}
-
- Intraoperative Ultrasound Guided Glioma Surgery; a Randomised, Controlled Trial. (US-GLIOMA). Ongoing study. May 2018. Contact author for more information.
Additional references
Black 1997
-
- Black PM, Moriarty T, Alexander E, Stieg P, Woodard EJ, Gleason PL, et al. Development and implementation of intraoperative magnetic resonance imaging and its neurosurgical applications. Neurosurgery 1997;41(4):831-45. - PubMed
Brignardello‐Petersen 2018
-
- Brignardello-Petersen R, Bonner A, Alexander PE, Siemieniuk RA, Furukawa TA, Rochwerg B, et al. Advances in the GRADE approach to rate the certainty in estimates from a network meta-analysis. Journal of Clinical Epidemiology 2018;93:36-44. - PubMed
Brignardello‐Petersen 2019a
-
- Brignardello-Petersen R, Mustafa RA, Siemieniuk RA, Murad MH, Agoritsas T, Izcovich A, et al, GRADE Working Group. GRADE approach to rate the certainty from a network meta-analysis: addressing incoherence. Journal of Clinical Epidemiology 2019;108:77-85. - PubMed
Brignardello‐Petersen 2019b
-
- Brignardello-Petersen R, Murad MH, Walter SD, McLeod S, Carrasco-Labra A, Rochwerg B, et al, GRADE Working Group. GRADE approach to rate the certainty from a network meta-analysis: avoiding spurious judgments of imprecision in sparse networks. Journal of Clinical Epidemiology 2019;105:60-7. - PubMed
Brodbelt 2015
-
- Brodbelt A, Greenberg D, Winters T, Williams M, Vernon S, Collins VP. Glioblastoma in England: 2007–2011. European Journal of Cancer 2015;51(4):533-42. - PubMed
Chaimani 2017
-
- Chaimani A, Caldwell DM, Li T, Higgins JP, Salanti G. Additional considerations are required when preparing a protocol for a systematic review with multiple interventions. Journal of Clinical Epidemiology 2017;83:65-74. - PubMed
Chang 2007
-
- Chang S, Vogelbaum M, Lang FF, Haines S, Kunwar S, Chiocca EA, et al. GNOSIS: guidelines for neuro-oncology: standards for investigational studies – reporting of surgically based therapeutic clinical trials. Journal of Neuro-oncology 2007;82(2):211-20. [PMID: ] - PubMed
Coburger 2019
-
- Coburger J, Wirtz CR. Fluorescence guided surgery by 5-ALA and intraoperative MRI in high grade glioma: a systematic review. Journal of Neuro-oncology 2019;141:533-46. - PubMed
Dirven 2014
Efthimiou 2016
-
- Efthimiou O, Debray TP, Valkenhoef G, Trelle S, Panayidou K, Moons KG, et al. GetReal in network meta-analysis: a review of the methodology. Research Synthesis Methods 2016;7(3):236-63. - PubMed
Eljamel 2016
-
- Eljamel MS, Mahboob SO. The effectiveness and cost-effectiveness of intraoperative imaging in high-grade glioma resection; a comparative review of intraoperative ALA, fluorescein, ultrasound and MRI. Photodiagnosis and Photodynamic Therapy 2016;16:35-43. [PMID: ] - PubMed
Esteves 2015a
Fountain 2016
GRADE Working Group 2004
Hall 2003
-
- Hall WA, Kowalik K, Liu H, Truwit CL, Kucharezyk J. Costs and benefits of intraoperative MR-guided brain tumor resection. Acta Neurochirurgica. Supplement 2003;85:137-42. [PMID: ] - PubMed
Hart 2019
Higgins 2019
-
- Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane Handbook for Systematic Reviews of Interventions version 6.0 (updated July 2019). Cochrane, 2019. Available from www.training.cochrane.org/handbook. - PMC - PubMed
Jenkinson 2018
Jiang 2017
Kowalik 2000
-
- Kowalik K, Truwit C, Hall W, Kucharczyk J. Initial assessment of costs and benefits of MRI-guided brain tumor resection. European Radiology 2000;10 Suppl 3:S366-7. [PMID: ] - PubMed
Louis 2016
-
- Louis DN, Perry A, Reifenberger G, Von Deimling A, Figarella-Branger D, Cavenee WK, et al. The 2016 World Health Organization classification of tumors of the central nervous system: a summary. Acta Neuropathologica 2016;131(6):803-20. - PubMed
Makary 2011
-
- Makary M, Chiocca EA, Erminy N, Antor M, Bergese SD, Abdel-Rasoul M, et al. Clinical and economic outcomes of low-field intraoperative MRI-guided tumor resection neurosurgery. Journal of Magnetic Resonance Imaging 2011;34(5):1022-30. [PMID: ] - PubMed
Meader 2014
Miwa 2004
-
- Miwa K, Shinoda J, Yano H, Okumura A, Iwama T, Nakashima T, et al. Discrepancy between lesion distributions on methionine PET and MR images in patients with glioblastoma multiforme: insight from a PET and MR fusion image study. Journal of Neurology, Neurosurgery, and Psychiatry 2004;75(10):1457-62. [PMID: ] - PMC - PubMed
NICE 2018
-
- National Institute for Health and Care Excellence. Brain tumours (primary) and brain metastases in adults (NG99). www.nice.org.uk/guidance/ng99 (accessed prior to 6 October 2020).
Parmar 1998
-
- Parmar MK, Torri V, Stewart L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Statistics in Medicine 1998;17(24):2815-34. - PubMed
Pichlmeier 2008
Puhan 2014
-
- Puhan MA, Schünemann HJ, Murad MH, Li T, Brignardello-Petersen R, Singh JA, et al, GRADE Working Group. A GRADE Working Group approach for rating the quality of treatment effect estimates from network meta-analysis. BMJ 2014;24(349):g5630. - PubMed
Review Manager 2014 [Computer program]
-
- Nordic Cochrane Centre, The Cochrane Collaboration Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Rücker 2015
Salanti 2011
-
- Salanti G, Ades AE, Ioannidis JP. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: an overview and tutorial. Journal of Clinical Epidemiology 2011;64(2):163-71. - PubMed
Salanti 2014
Sawaya 1998
-
- Sawaya R, Hammoud M, Schoppa D, Hess KR, Wu SZ, Shi WM, et al. Neurosurgical outcomes in a modern series of 400 craniotomies for treatment of parenchymal tumors. Neurosurgery 1998;42:1044-56. - PubMed
Schulder 2003
-
- Schulder M, Carmel PW. Intraoperative magnetic resonance imaging: impact on brain tumor surgery. Cancer Control 2003;10(2):115-24. [PMID: ] - PubMed
Slof 2015
-
- Slof J, DÃÂez Valle R, Galván J. Cost-effectiveness of 5-aminolevulinic acid-induced fluorescence in malignant glioma surgery. Neurologia (Barcelona, Spain) 2015;30(3):163-8. [PMID: ] - PubMed
Stata [Computer program]
-
- Stata. Version 15. College Station, TX, USA: StataCorp, 2017. Available at www.stata.com.
Stummer 1998
-
- Stummer W, Stocker S, Wagner S, Stepp H, Fritsch C, Goetz C, et al. Intraoperative detection of malignant gliomas by 5-aminolevulinic acid- induced porphyrin fluorescence. Neurosurgery 1998;42(3):518-26. - PubMed
Stummer 2000
-
- Stummer W, Novotny A, Stepp H, Goetz C, Bise K, Reulen HJ. Fluorescence-guided resection of glioblastoma multiforme by using 5-aminolevulinic acid-induced porphyrins: a prospective study in 52 consecutive patients. Journal of Neurosurgery 2000;93(6):1003-13. - PubMed
Stupp 2005
-
- Stupp R, Mason WP, den Bent MJ, Weller M, Fisher B, Taphoorn MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. New England Journal of Medicine 2005;352(10):987-96. [PMID: ] - PubMed
Wen 2010
-
- Wen PY, Macdonald DR, Reardon DA, Cloughesy TF, Sorensen AG, Galanis E, et al. Updated response assessment criteria for high-grade gliomas: response assessment in neuro-oncology working group. Journal of Clinical Oncology 2010;28(11):1963-72. - PubMed
References to other published versions of this review
Fountain 2020
-
- Fountain DM, Jenkinson MD, Bryant A, Vale L, Bulbeck H, Hart MG, et al. Intraoperative imaging technology to maximise extent of resection for glioma: a network meta-analysis. Cochrane Database of Systematic Reviews 2020, Issue 5. Art. No: CD013630. [DOI: 10.1002/14651858.CD013630] - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical