

Leadless pacemaker implant with concomitant atrioventricular node ablation: Experience with the Micra transcatheter pacemaker
- PMID: 33428248
- PMCID: PMC7986103
- DOI: 10.1111/jce.14881
Leadless pacemaker implant with concomitant atrioventricular node ablation: Experience with the Micra transcatheter pacemaker
Abstract
Background: The feasibility and outcomes of concomitant atrioventricular node ablation (AVNA) and leadless pacemaker implant are not well studied. We report outcomes in patients undergoing Micra implant with concomitant AVNA.
Methods: Patients undergoing AVNA at the time of Micra implant from the Micra Transcatheter Pacing (IDE) Study, Continued Access (CA) study, and Post-Approval Registry (PAR) were included in the analysis and compared to Micra patients without AVNA. Baseline characteristics, acute and follow-up outcomes, and electrical performance were compared between patients with and without AVNA during the follow-up period.
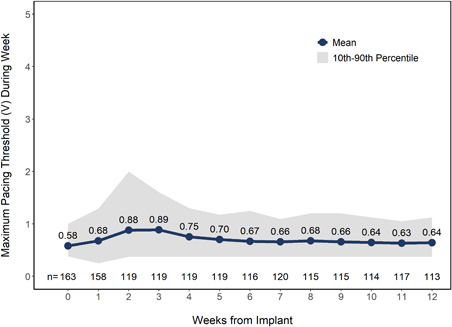
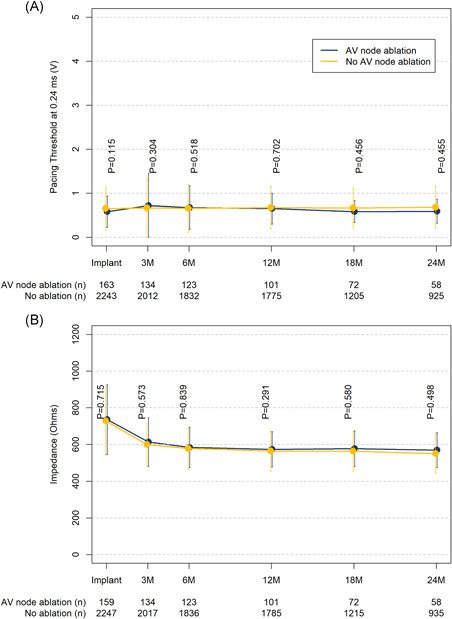
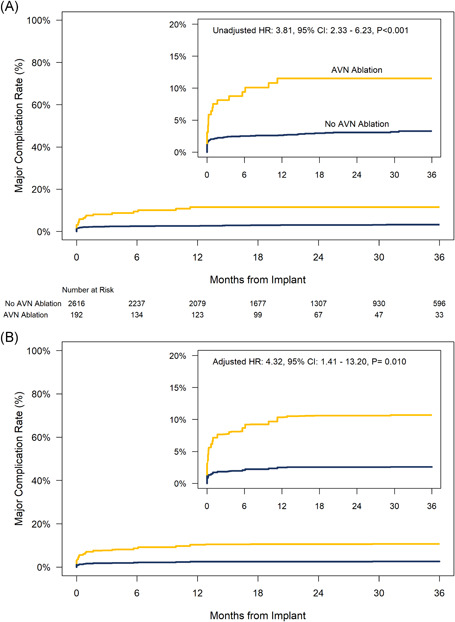
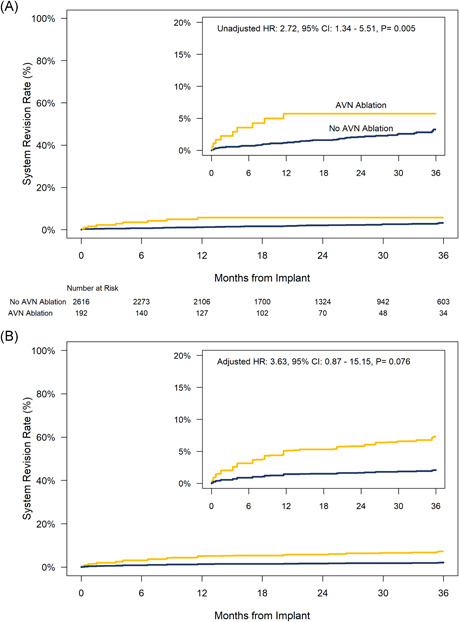
Results: A total of 192 patients (mean age 77.4 ± 8.9 years, 72% female) underwent AVNA at the time of Micra implant and were followed for 20.4 ± 15.6 months. AVNA patients were older, more frequently female, and tended to have more co-morbid conditions compared with non-AVNA patients (N = 2616). Implant was successful in 191 of 192 patients (99.5%). The mean pacing threshold at implant was 0.58 ± 0.35 V and remained stable during follow-up. Major complications within 30 days occurred more frequently in AVNA patients than non-AVNA patients (7.3% vs. 2.0%, p < .001). The risk of major complications through 36-months was higher in AVNA patients (hazard ratio: 3.81, 95% confidence interval: 2.33-6.23, p < .001). Intermittent loss of capture occurred in three AVNA patients (1.6%), all were within 30 days of implant and required system revision. There were no device macrodislodgements or unexpected device malfunctions.
Conclusion: Concomitant AVN ablation and leadless pacemaker implant is feasible. Pacing thresholds are stable over time. However, patient comorbidities and the risk of major complications are higher in patients undergoing AVNA.
Trial registration: ClinicalTrials.gov NCT02536118 NCT02488681 NCT02004873.
Keywords: AV node ablation; Micra; leadless pacemaker.
© 2021 The Authors. Journal of Cardiovascular Electrophysiology Published by Wiley Periodicals LLC.
Figures
Similar articles
-
Concurrent Micra Leadless Pacemaker Implantation and AVN Ablation: Computer Modeling of Novel Risk Mitigation Strategy.Pacing Clin Electrophysiol. 2025 Mar;48(3):287-293. doi: 10.1111/pace.15149. Epub 2025 Jan 27. Pacing Clin Electrophysiol. 2025. PMID: 39869004 Free PMC article. Review.
-
A leadless ventricular pacemaker providing atrioventricular synchronous pacing in the real-world setting: 12-Month results from the Micra AV post-approval registry.Heart Rhythm. 2024 Oct;21(10):1939-1947. doi: 10.1016/j.hrthm.2024.06.008. Epub 2024 Jun 13. Heart Rhythm. 2024. PMID: 38878939
-
Leadless Pacemaker Implantation in Hemodialysis Patients: Experience With the Micra Transcatheter Pacemaker.JACC Clin Electrophysiol. 2019 Feb;5(2):162-170. doi: 10.1016/j.jacep.2018.12.008. Epub 2019 Jan 30. JACC Clin Electrophysiol. 2019. PMID: 30784685
-
Safety and Efficacy Outcomes of Combined Leadless Pacemaker and Atrioventricular Nodal Ablation for Atrial Fibrillation Using a Single Femoral Puncture Approach.Heart Lung Circ. 2020 May;29(5):759-765. doi: 10.1016/j.hlc.2019.05.100. Epub 2019 May 27. Heart Lung Circ. 2020. PMID: 31208898
-
Design and evaluation of the Micra Transcatheter Pacing System for bradyarrhythmia management.Future Cardiol. 2019 Jan;15(1):9-15. doi: 10.2217/fca-2018-0077. Epub 2018 Dec 5. Future Cardiol. 2019. PMID: 30516083 Review.
Cited by
-
Atrioventricular synchronous leadless pacing: Micra AV.Cardiol J. 2024;31(1):147-155. doi: 10.5603/CJ.a2023.0035. Epub 2023 May 29. Cardiol J. 2024. PMID: 37246458 Free PMC article. Review.
-
Concurrent Micra Leadless Pacemaker Implantation and AVN Ablation: Computer Modeling of Novel Risk Mitigation Strategy.Pacing Clin Electrophysiol. 2025 Mar;48(3):287-293. doi: 10.1111/pace.15149. Epub 2025 Jan 27. Pacing Clin Electrophysiol. 2025. PMID: 39869004 Free PMC article. Review.
-
Leadless Pacemakers: State of the Art and Selection of the Ideal Candidate.Curr Cardiol Rev. 2023;19(5):43-50. doi: 10.2174/1573403X19666230331094647. Curr Cardiol Rev. 2023. PMID: 36999695 Free PMC article. Review.
References
-
- Lee SH, Chen SA, Tai CT, et al. Comparisons of quality of life and cardiac performance after complete atrioventricular junction ablation and atrioventricular junction modification in patients with medically refractory atrial fibrillation. J Am Coll Cardiol. 1998;31(3):637‐644. - PubMed
-
- Kay GN, Ellenbogen KA, Giudici M, et al. The Ablate and Pace Trial: a prospective study of catheter ablation of the AV conduction system and permanent pacemaker implantation for treatment of atrial fibrillation. APT Investigators. J Interv Card Electrophysiol. 1998;2(2):121‐135. - PubMed
-
- Hoffmayer KS, Scheinman M. Current role of atrioventricular junction (AVJ) ablation. Pacing Clin Electrophysiol. 2013;36(2):257‐265. - PubMed
-
- Kuck KH, Brugada J, Fürnkranz A, et al. Cryoballoon or radiofrequency ablation for paroxysmal atrial fibrillation. N Engl J Med. 2016;374(23):2235‐2245. - PubMed
-
- Cantillon DJ, Exner DV, Badie N, et al. Complications and health care costs associated with transvenous cardiac pacemakers in a nationwide assessment. JACC Clin Electrophysiol. 2017;3(11):1296‐1305. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
