

The Sensitivity and Costs of Testing for SARS-CoV-2 Infection With Saliva Versus Nasopharyngeal Swabs : A Systematic Review and Meta-analysis
- PMID: 33428446
- PMCID: PMC7822569
- DOI: 10.7326/M20-6569
The Sensitivity and Costs of Testing for SARS-CoV-2 Infection With Saliva Versus Nasopharyngeal Swabs : A Systematic Review and Meta-analysis
Erratum in
-
Correction: The Sensitivity and Costs of Testing for SARS-CoV-2 Infection With Saliva Versus Nasopharyngeal Swabs.Ann Intern Med. 2021 Apr;174(4):584. doi: 10.7326/L21-0055. Ann Intern Med. 2021. PMID: 33872527 No abstract available.
Abstract
Background: Nasopharyngeal swabs are the primary sampling method used for detection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), but they require a trained health care professional and extensive personal protective equipment.
Purpose: To determine the difference in sensitivity for SARS-CoV-2 detection between nasopharyngeal swabs and saliva and estimate the incremental cost per additional SARS-CoV-2 infection detected with nasopharyngeal swabs.
Data sources: Embase, Medline, medRxiv, and bioRxiv were searched from 1 January to 1 November 2020. Cost inputs were from nationally representative sources in Canada and were converted to 2020 U.S. dollars.
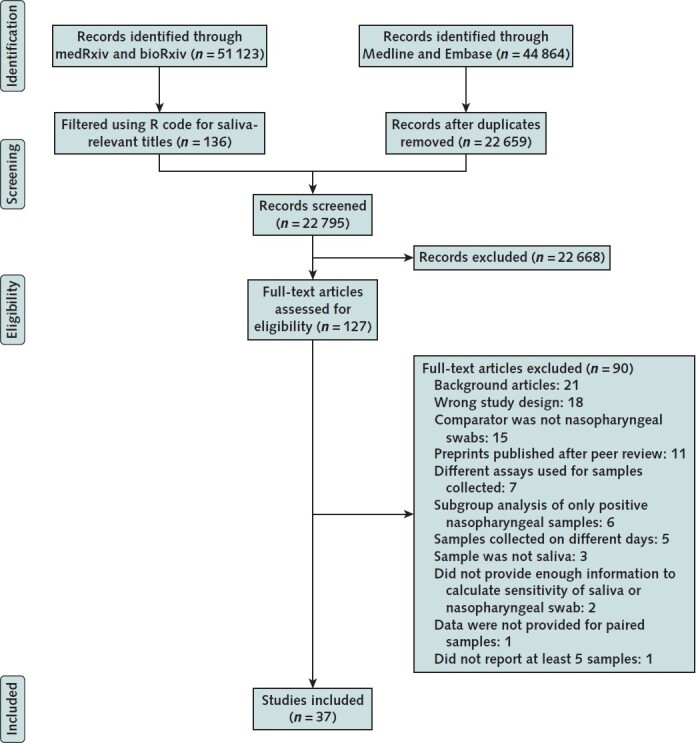
Study selection: Studies including at least 5 paired nasopharyngeal swab and saliva samples and reporting diagnostic accuracy for SARS-CoV-2 detection.
Data extraction: Data were independently extracted using standardized forms, and study quality was assessed using QUADAS-2 (Quality Assessment of Diagnostic Accuracy Studies 2).
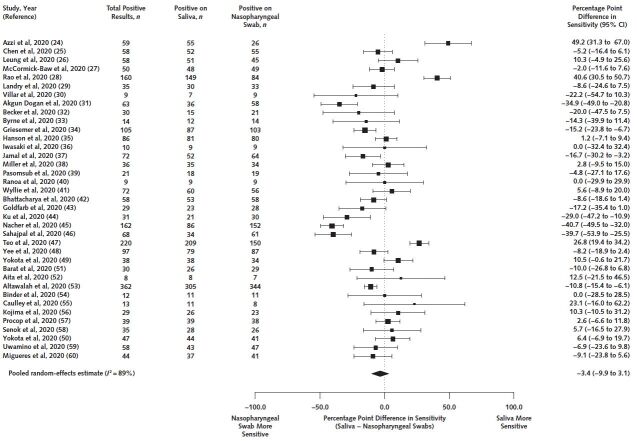
Data synthesis: Thirty-seven studies with 7332 paired samples were included. Against a reference standard of a positive result on either sample, the sensitivity of saliva was 3.4 percentage points lower (95% CI, 9.9 percentage points lower to 3.1 percentage points higher) than that of nasopharyngeal swabs. Among persons with previously confirmed SARS-CoV-2 infection, saliva's sensitivity was 1.5 percentage points higher (CI, 7.3 percentage points lower to 10.3 percentage points higher) than that of nasopharyngeal swabs. Among persons without a previous SARS-CoV-2 diagnosis, saliva was 7.9 percentage points less (CI, 14.7 percentage points less to 0.8 percentage point more) sensitive. In this subgroup, if testing 100 000 persons with a SARS-CoV-2 prevalence of 1%, nasopharyngeal swabs would detect 79 more (95% uncertainty interval, 5 fewer to 166 more) persons with SARS-CoV-2 than saliva, but with an incremental cost per additional infection detected of $8093.
Limitation: The reference standard was imperfect, and saliva collection procedures varied.
Conclusion: Saliva sampling seems to be a similarly sensitive and less costly alternative that could replace nasopharyngeal swabs for collection of clinical samples for SARS-CoV-2 testing.
Primary funding source: McGill Interdisciplinary Initiative in Infection and Immunity. (PROSPERO: CRD42020203415).
Conflict of interest statement
Figures
Comment in
-
The Sensitivity and Costs of Testing for SARS-CoV-2 Infection With Saliva Versus Nasopharyngeal Swabs.Ann Intern Med. 2021 Apr;174(4):582. doi: 10.7326/L21-0092. Ann Intern Med. 2021. PMID: 33872539 No abstract available.
-
Saliva and nasopharyngeal samples have similar sensitivity for detecting SARS-CoV-2.Ann Intern Med. 2021 May;174(5):JC55. doi: 10.7326/ACPJ202105180-055. Epub 2021 May 4. Ann Intern Med. 2021. PMID: 33939482
References
-
- Johns Hopkins Coronavirus Resource Center. COVID-19 map. Accessed at https://coronavirus.jhu.edu/map.html on 16 December 2020.
-
- Alberta Health Services. IPC recommendations PPE table for assessment centres during COVID-19. Updated 18 December 2020. Accessed at www.albertahealthservices.ca/assets/healthinfo/ipc/hi-ipc-assmt-cntrs-co... on 17 September 2020.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous