

COVID-19 and multisystem inflammatory syndrome in children: A systematic review and meta-analysis
- PMID: 33428826
- PMCID: PMC8013394
- DOI: 10.1002/ppul.25245
COVID-19 and multisystem inflammatory syndrome in children: A systematic review and meta-analysis
Abstract
Background: Multisystem inflammatory syndrome in children (MIS-C) associated with coronavirus disease 2019 has been increasingly recognized. However, the clinical features of MIS-C and the differences from Kawasaki disease remain unknown. The study aims to investigate the epidemiology and clinical course of MIS-C.
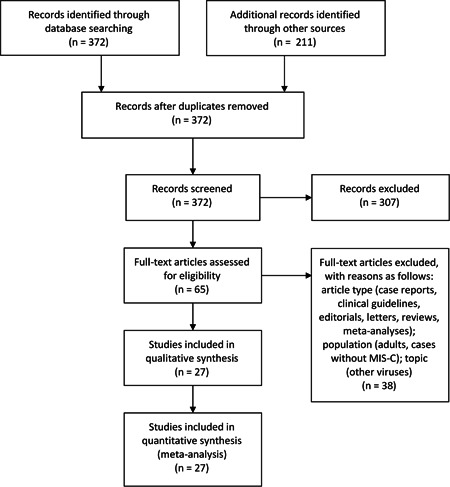
Methods: PubMed and EMBASE were searched through August 30, 2020. Observational studies describing MIS-C were included. Data regarding demographic features, clinical symptoms, laboratory, echocardiography and radiology findings, treatments, and outcomes were extracted. Study-specific estimates were combined using one-group meta-analysis in a random-effects model.
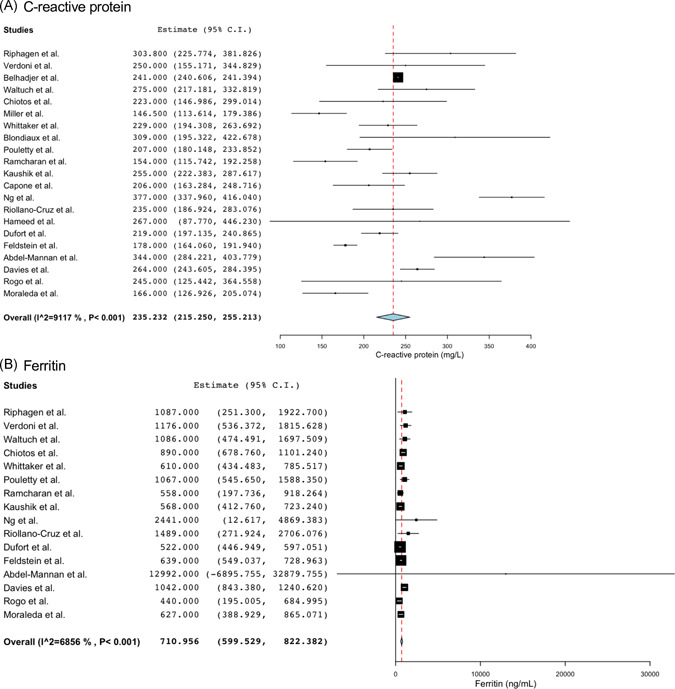
Results: A total of 27 studies were identified including 917 MIS-C patients. The mean age was 9.3 (95% confidence interval [CI], 8.4-10.1). The pooled proportions of Hispanic and Black cases were 34.6% (95% CI, 28.3-40.9) and 31.5% (95% CI, 24.8-38.1), respectively. The common manifestations were gastrointestinal symptoms (87.3%; 95% CI, 82.9-91.6) and cardiovascular involvement such as myocardial dysfunction (55.3%; 95% CI, 42.4-68.2), coronary artery aneurysms (21.7%; 95% CI, 12.8-30.1) and shock (65.8%; 95% CI, 51.1-80.4), with marked elevated inflammatory and cardiac markers. The majority of patients received intravenous immunoglobulin (81.0%; 95% CI, 75.0-86.9), aspirin (67.3%; 95% CI, 48.8-85.7), and corticosteroids (63.6%; 95% CI, 53.4-73.8) with a variety of anti-inflammatory agents. Although myocardial dysfunction improved in 55.1% (95% CI, 33.4-76.8) at discharge, the rate of extracorporeal membrane oxygenation use was 6.3% (95% CI, 2.8-9.8) and the mortality was 1.9% (95% CI, 1.0-2.8).
Conclusion: Our findings suggest that MIS-C leads to multiple organ failure, including gastrointestinal manifestations, myocardial dysfunction and coronary abnormalities, and has distinct features from Kawasaki disease.
Keywords: Kawasaki disease; MIS-C; PIMS-TS; hyperinflammatory shock; myocarditis.
© 2020 Wiley Periodicals LLC.
Conflict of interest statement
The authors declare that there are no conflict of interests.
Figures



Comment on
-
Multi-system inflammatory syndrome in children & adolescents (MIS-C): A systematic review of clinical features and presentation.Paediatr Respir Rev. 2021 Jun;38:51-57. doi: 10.1016/j.prrv.2020.08.001. Epub 2020 Aug 11. Paediatr Respir Rev. 2021. PMID: 32891582 Free PMC article.
References
-
- Castagnoli R, Votto M, Licari A, et al. Severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2) infection in children and adolescents: a systematic review. JAMA pediatrics. 2020;174(9):882‐889. - PubMed
-
- Yasuhara J, Kuno T, Takagi H, Sumitomo N. Clinical characteristics of COVID‐19 in children: a systematic review. Pediatr Pulmonol. 2020;55:2565‐2575. - PubMed
-
- Centers for Disease Control and Prevention . Multisystem inflammatory syndrome in children (MIS‐C) associated with coronavirus disease 2019 (COVID‐19). 2020. https://emergency.cdc.gov/han/2020/han00432.asp. Accessed June 20, 2020.
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
