

Prevalence and risk factors for delirium in critically ill patients with COVID-19 (COVID-D): a multicentre cohort study
- PMID: 33428871
- PMCID: PMC7832119
- DOI: 10.1016/S2213-2600(20)30552-X
Prevalence and risk factors for delirium in critically ill patients with COVID-19 (COVID-D): a multicentre cohort study
Erratum in
-
Correction to Lancet Respir Med 2021; published online Jan 8. https://doi.org/10.1016/S2213-2600(20)30552-X.Lancet Respir Med. 2021 Mar;9(3):e29. doi: 10.1016/S2213-2600(21)00047-3. Epub 2021 Jan 27. Lancet Respir Med. 2021. PMID: 33515501 Free PMC article. No abstract available.
Abstract
Background: To date, 750 000 patients with COVID-19 worldwide have required mechanical ventilation and thus are at high risk of acute brain dysfunction (coma and delirium). We aimed to investigate the prevalence of delirium and coma, and risk factors for delirium in critically ill patients with COVID-19, to aid the development of strategies to mitigate delirium and associated sequelae.
Methods: This multicentre cohort study included 69 adult intensive care units (ICUs), across 14 countries. We included all patients (aged ≥18 years) admitted to participating ICUs with severe acute respiratory syndrome coronavirus 2 infection before April 28, 2020. Patients who were moribund or had life-support measures withdrawn within 24 h of ICU admission, prisoners, patients with pre-existing mental illness, neurodegenerative disorders, congenital or acquired brain damage, hepatic coma, drug overdose, suicide attempt, or those who were blind or deaf were excluded. We collected de-identified data from electronic health records on patient demographics, delirium and coma assessments, and management strategies for a 21-day period. Additional data on ventilator support, ICU length of stay, and vital status was collected for a 28-day period. The primary outcome was to determine the prevalence of delirium and coma and to investigate any associated risk factors associated with development of delirium the next day. We also investigated predictors of number of days alive without delirium or coma. These outcomes were investigated using multivariable regression.
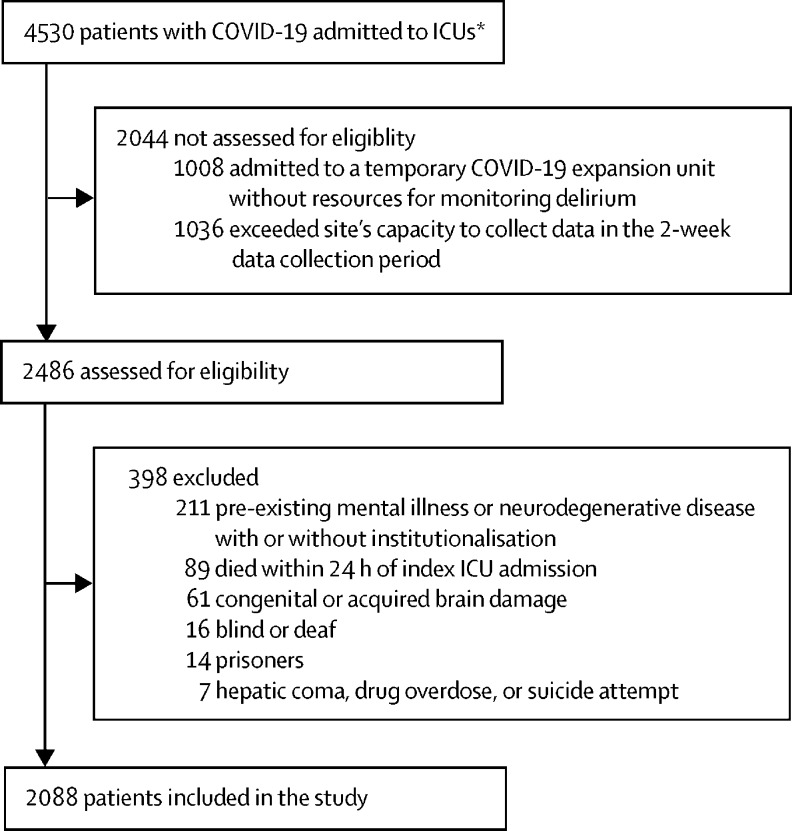
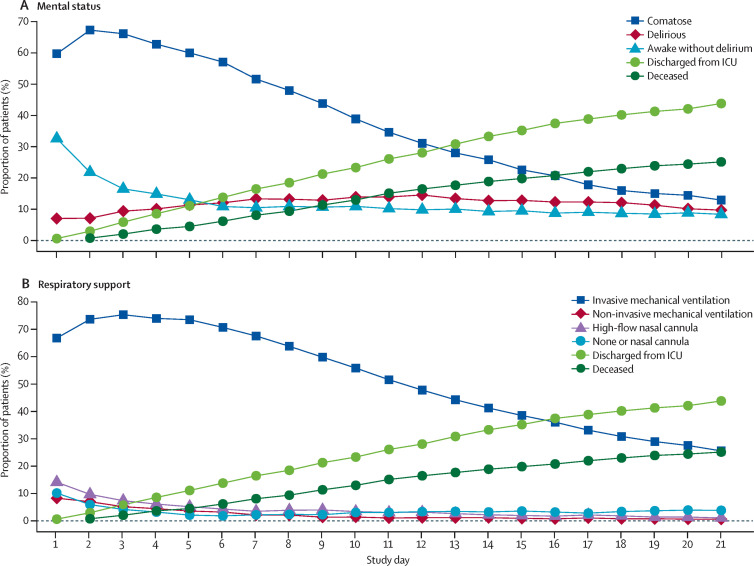
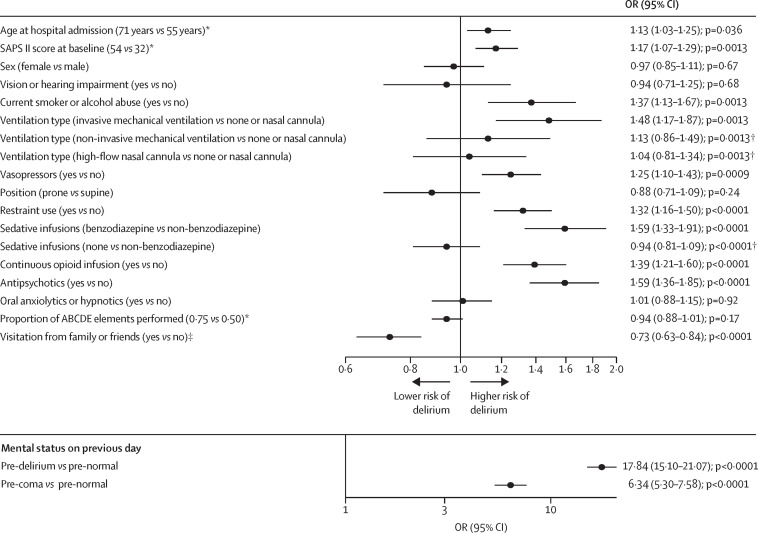
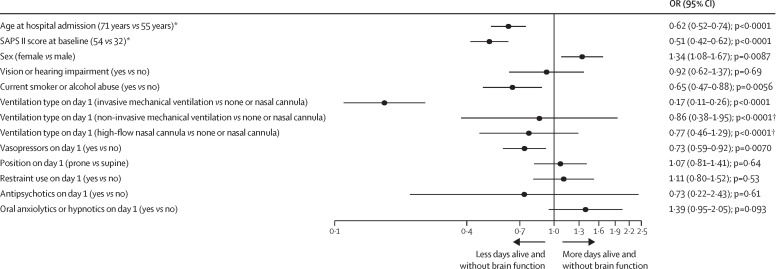
Findings: Between Jan 20 and April 28, 2020, 4530 patients with COVID-19 were admitted to 69 ICUs, of whom 2088 patients were included in the study cohort. The median age of patients was 64 years (IQR 54 to 71) with a median Simplified Acute Physiology Score (SAPS) II of 40·0 (30·0 to 53·0). 1397 (66·9%) of 2088 patients were invasively mechanically ventilated on the day of ICU admission and 1827 (87·5%) were invasively mechanical ventilated at some point during hospitalisation. Infusion with sedatives while on mechanical ventilation was common: 1337 (64·0%) of 2088 patients were given benzodiazepines for a median of 7·0 days (4·0 to 12·0) and 1481 (70·9%) were given propofol for a median of 7·0 days (4·0 to 11·0). Median Richmond Agitation-Sedation Scale score while on invasive mechanical ventilation was -4 (-5 to -3). 1704 (81·6%) of 2088 patients were comatose for a median of 10·0 days (6·0 to 15·0) and 1147 (54·9%) were delirious for a median of 3·0 days (2·0 to 6·0). Mechanical ventilation, use of restraints, and benzodiazepine, opioid, and vasopressor infusions, and antipsychotics were each associated with a higher risk of delirium the next day (all p≤0·04), whereas family visitation (in person or virtual) was associated with a lower risk of delirium (p<0·0001). During the 21-day study period, patients were alive without delirium or coma for a median of 5·0 days (0·0 to 14·0). At baseline, older age, higher SAPS II scores, male sex, smoking or alcohol abuse, use of vasopressors on day 1, and invasive mechanical ventilation on day 1 were independently associated with fewer days alive and free of delirium and coma (all p<0·01). 601 (28·8%) of 2088 patients died within 28 days of admission, with most of those deaths occurring in the ICU.
Interpretation: Acute brain dysfunction was highly prevalent and prolonged in critically ill patients with COVID-19. Benzodiazepine use and lack of family visitation were identified as modifiable risk factors for delirium, and thus these data present an opportunity to reduce acute brain dysfunction in patients with COVID-19.
Funding: None.
Translations: For the French and Spanish translations of the abstract see Supplementary Materials section.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Sedation in mechanically ventilated patients with COVID-19.Lancet Respir Med. 2021 Mar;9(3):218-219. doi: 10.1016/S2213-2600(20)30570-1. Epub 2021 Jan 8. Lancet Respir Med. 2021. PMID: 33428873 Free PMC article. No abstract available.
References
-
- WHO Coronavirus disease (COVID-2019). Situation report–126. May 25, 2020. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situatio...
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
