

Validation of Risk Prediction Models to Inform Clinical Decisions After Acute Kidney Injury
- PMID: 33428996
- PMCID: PMC8234511
- DOI: 10.1053/j.ajkd.2020.12.008
Validation of Risk Prediction Models to Inform Clinical Decisions After Acute Kidney Injury
Abstract
Rationale & objective: There is limited evidence to guide follow-up after acute kidney injury (AKI). Knowledge gaps include which patients to prioritize, at what time point, and for mitigation of which outcomes. In this study, we sought to compare the net benefit of risk model-based clinical decisions following AKI.
Study design: External validation of 2 risk models of AKI outcomes: the Grampian -Aberdeen (United Kingdom) AKI readmissions model and the Alberta (Canada) kidney disease risk model of chronic kidney disease (CKD) glomerular (G) filtration rate categories 4 and 5 (CKD G4 and G5). Process mining to delineate existing care pathways.
Setting & participants: Validation was based on data from adult hospital survivors of AKI from Grampian, 2011-2013.
Predictors: KDIGO-based measures of AKI severity and comorbidities specified in the original models.
Outcomes: Death or readmission within 90 days for all hospital survivors. Progression to new CKD G4-G5 for patients surviving at least 90 days after AKI.
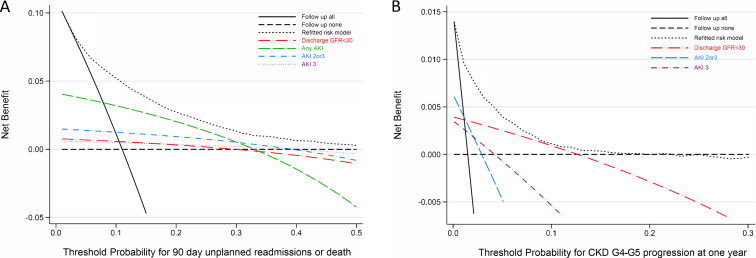
Analytical approach: Decision curve analysis to assess the "net benefit" of use of risk models to guide clinical care compared to alternative approaches (eg, prioritizing all AKI, severe AKI, or only those without kidney recovery).
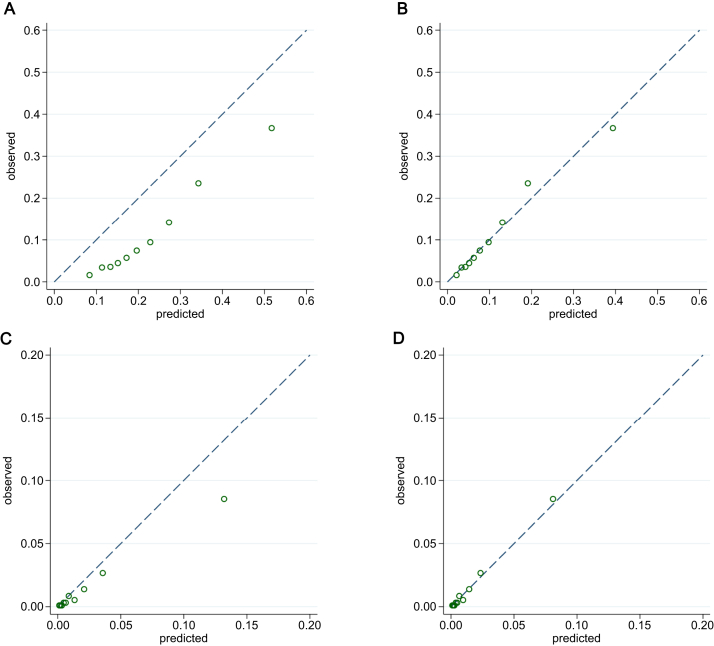
Results: 26,575 of 105,461 hospital survivors in Grampian (mean age, 60.9 ± 19.8 [SD] years) were included for validation of the death or readmission model, and 9,382 patients (mean age, 60.9 ± 19.8 years) for the CKD G4-G5 model. Both models discriminated well (area under the curve [AUC], 0.77 and 0.86, respectively). Decision curve analysis showed greater net benefit for follow up of all AKI than only severe AKI in most cases. Both original and refitted models provided net benefit superior to any other decision strategy. In process mining of all hospital discharges, 41% of readmissions and deaths occurred among people recovering after AKI. 1,464 of 3,776 people (39%) readmitted after AKI had received no intervening monitoring.
Limitations: Both original models overstated risks, indicating a need for regular updating.
Conclusions: Follow up after AKI has potential net benefit for preempting readmissions, death, and subsequent CKD progression. Decisions could be improved by using risk models and by focusing on AKI across a full spectrum of severity. The current lack of monitoring among many with poor outcomes indicates possible opportunities for implementation of decision support.
Keywords: CKD progression; CKD surveillance; acute kidney injury (AKI); chronic kidney disease (CKD); death; follow-up care; hospital readmission; model-guided decisions; mortality; net benefit; post-AKI care; post-discharge monitoring; risk prediction.
Copyright © 2021 The Authors. Published by Elsevier Inc. All rights reserved.
Figures

Comment in
-
We Won't Get Fooled Again: Finding the Who to Follow After Acute Kidney Injury.Am J Kidney Dis. 2021 Jul;78(1):16-18. doi: 10.1053/j.ajkd.2021.02.325. Epub 2021 Apr 27. Am J Kidney Dis. 2021. PMID: 33931275 No abstract available.
Similar articles
-
Processes of Care After Hospital Discharge for Survivors of Acute Kidney Injury: A Population-Based Cohort Study.Am J Kidney Dis. 2024 Feb;83(2):216-228. doi: 10.1053/j.ajkd.2023.07.015. Epub 2023 Sep 19. Am J Kidney Dis. 2024. PMID: 37734688
-
Acute kidney injury as an independent risk factor for unplanned 90-day hospital readmissions.BMC Nephrol. 2017 Jan 6;18(1):9. doi: 10.1186/s12882-016-0430-4. BMC Nephrol. 2017. PMID: 28061831 Free PMC article.
-
Real-Time Clinical Decision Support Based on Recurrent Neural Networks for In-Hospital Acute Kidney Injury: External Validation and Model Interpretation.J Med Internet Res. 2021 Apr 16;23(4):e24120. doi: 10.2196/24120. J Med Internet Res. 2021. PMID: 33861200 Free PMC article.
-
Preoperative risk prediction models for acute kidney injury after noncardiac surgery: an independent external validation cohort study.Br J Anaesth. 2024 Sep;133(3):508-518. doi: 10.1016/j.bja.2024.02.018. Epub 2024 Mar 24. Br J Anaesth. 2024. PMID: 38527923
-
Predicting progression to chronic kidney disease after recovery from acute kidney injury.Curr Opin Nephrol Hypertens. 2012 Nov;21(6):628-34. doi: 10.1097/MNH.0b013e3283588f24. Curr Opin Nephrol Hypertens. 2012. PMID: 23010757 Review.
Cited by
-
Predicting the risks of kidney failure and death in adults with moderate to severe chronic kidney disease: multinational, longitudinal, population based, cohort study.BMJ. 2024 Apr 15;385:e078063. doi: 10.1136/bmj-2023-078063. BMJ. 2024. PMID: 38621801 Free PMC article.
-
Biomarker Panels for Predicting Progression of Kidney Disease in Acute Kidney Injury Survivors.Clin J Am Soc Nephrol. 2025 Mar 1;20(3):337-345. doi: 10.2215/CJN.0000000622. Epub 2024 Dec 13. Clin J Am Soc Nephrol. 2025. PMID: 39671257
-
Cost-effectiveness and value of information analysis of NephroCheck and NGAL tests compared to standard care for the diagnosis of acute kidney injury.BMC Nephrol. 2021 Dec 1;22(1):399. doi: 10.1186/s12882-021-02610-9. BMC Nephrol. 2021. PMID: 34852765 Free PMC article.
-
Nephrologist's Perceptions of Risk of Severe Chronic Kidney Disease and Outpatient Follow-up After Hospitalization With AKI: Multinational Randomized Survey Study.Can J Kidney Health Dis. 2025 Apr 30;12:20543581251336548. doi: 10.1177/20543581251336548. eCollection 2025. Can J Kidney Health Dis. 2025. PMID: 40321680 Free PMC article.
-
Expectation of clinical decision support systems: a survey study among nephrologist end-users.BMC Med Inform Decis Mak. 2023 Oct 26;23(1):239. doi: 10.1186/s12911-023-02317-x. BMC Med Inform Decis Mak. 2023. PMID: 37884906 Free PMC article.
References
-
- Thakar C.V., Parikh P.J., Liu Y. Acute kidney injury (AKI) and risk of readmissions in patients with heart failure. Am J Cardiol. 2012;109(10):1482–1486. - PubMed
-
- Silver S.A., Harel Z., McArthur E. 30-day readmissions after an acute kidney injury hospitalization. Am J Med. 2017;130(2):163–172. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
