

Circuits between infected macrophages and T cells in SARS-CoV-2 pneumonia
- PMID: 33429418
- PMCID: PMC7987233
- DOI: 10.1038/s41586-020-03148-w
Circuits between infected macrophages and T cells in SARS-CoV-2 pneumonia
Abstract
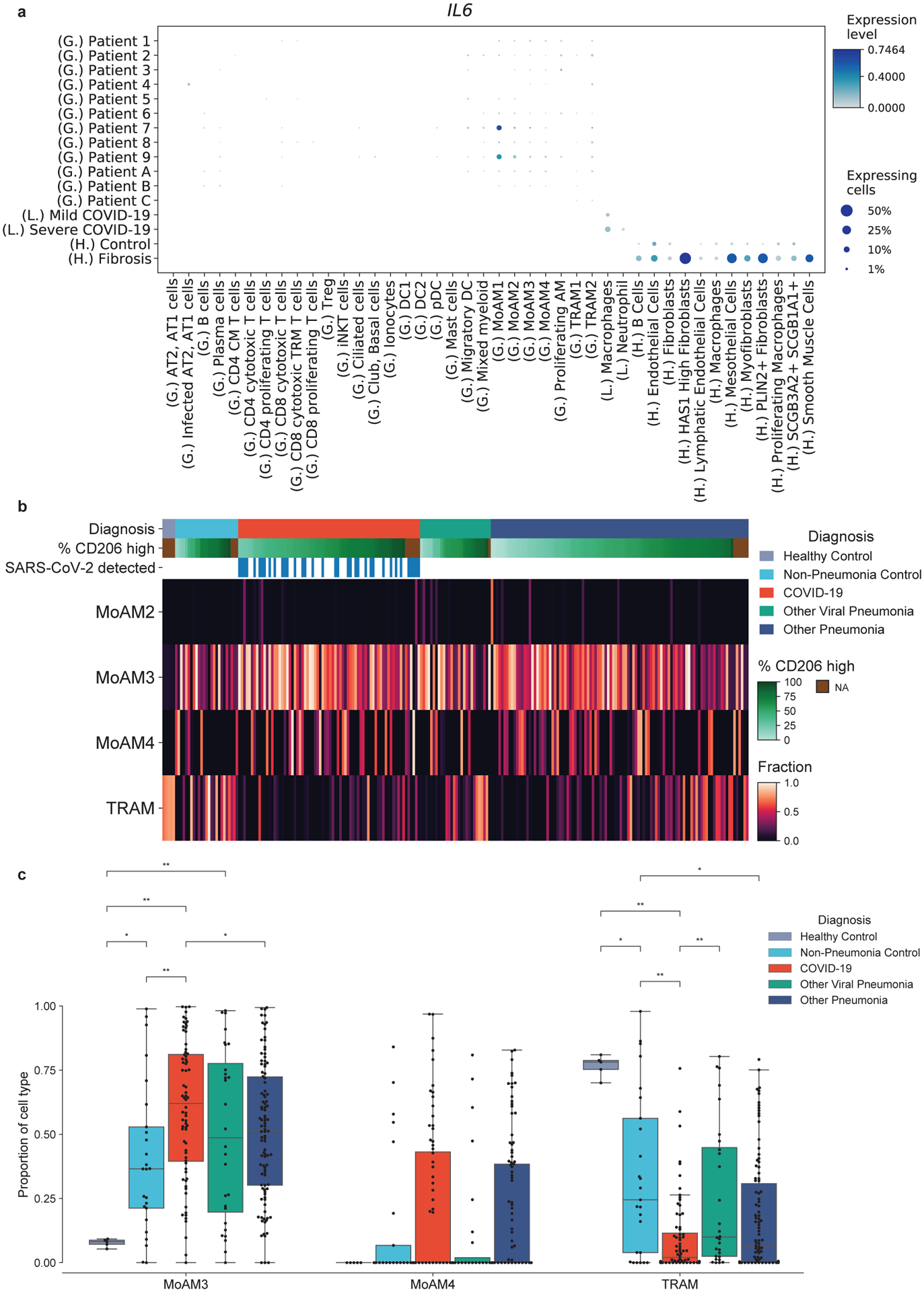
Some patients infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) develop severe pneumonia and acute respiratory distress syndrome1 (ARDS). Distinct clinical features in these patients have led to speculation that the immune response to virus in the SARS-CoV-2-infected alveolus differs from that in other types of pneumonia2. Here we investigate SARS-CoV-2 pathobiology by characterizing the immune response in the alveoli of patients infected with the virus. We collected bronchoalveolar lavage fluid samples from 88 patients with SARS-CoV-2-induced respiratory failure and 211 patients with known or suspected pneumonia from other pathogens, and analysed them using flow cytometry and bulk transcriptomic profiling. We performed single-cell RNA sequencing on 10 bronchoalveolar lavage fluid samples collected from patients with severe coronavirus disease 2019 (COVID-19) within 48 h of intubation. In the majority of patients with SARS-CoV-2 infection, the alveolar space was persistently enriched in T cells and monocytes. Bulk and single-cell transcriptomic profiling suggested that SARS-CoV-2 infects alveolar macrophages, which in turn respond by producing T cell chemoattractants. These T cells produce interferon-γ to induce inflammatory cytokine release from alveolar macrophages and further promote T cell activation. Collectively, our results suggest that SARS-CoV-2 causes a slowly unfolding, spatially limited alveolitis in which alveolar macrophages containing SARS-CoV-2 and T cells form a positive feedback loop that drives persistent alveolar inflammation.
Conflict of interest statement
Authors do not declare conflict of interest.
Figures










Update of
-
Alveolitis in severe SARS-CoV-2 pneumonia is driven by self-sustaining circuits between infected alveolar macrophages and T cells.bioRxiv [Preprint]. 2020 Aug 7:2020.08.05.238188. doi: 10.1101/2020.08.05.238188. bioRxiv. 2020. Update in: Nature. 2021 Feb;590(7847):635-641. doi: 10.1038/s41586-020-03148-w. PMID: 34013276 Free PMC article. Updated. Preprint.
Comment in
-
Signs of self-sustained inflammatory circuits in severe COVID pneumonia.Nature. 2021 Feb;590(7847):553-554. doi: 10.1038/d41586-021-00296-5. Nature. 2021. PMID: 33558748 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
- I01 CX001777/CX/CSRD VA/United States
- HL147290/NH/NIH HHS/United States
- R01 HL131745/HL/NHLBI NIH HHS/United States
- S10 OD011996/OD/NIH HHS/United States
- P01 AG049665/AG/NIA NIH HHS/United States
- U19 AI135964/AI/NIAID NIH HHS/United States
- P30 CA060553/CA/NCI NIH HHS/United States
- HL14578/NH/NIH HHS/United States
- R01 HL145478/HL/NHLBI NIH HHS/United States
- R01 HL147575/HL/NHLBI NIH HHS/United States
- R56 HL135124/HL/NHLBI NIH HHS/United States
- R01 HL134800/HL/NHLBI NIH HHS/United States
- GM129312/NH/NIH HHS/United States
- HL134800/NH/NIH HHS/United States
- K08 HL159356/HL/NHLBI NIH HHS/United States
- L30 CA153420/CA/NCI NIH HHS/United States
- K08 HL128867/HL/NHLBI NIH HHS/United States
- 1S10OD011996-01/NH/NIH HHS/United States
- R01 HL153312/HL/NHLBI NIH HHS/United States
- UL1 TR001422/TR/NCATS NIH HHS/United States
- T32 AG020506/AG/NIA NIH HHS/United States
- K99 AG068544/AG/NIA NIH HHS/United States
- HL147575/NH/NIH HHS/United States
- R01 HL147290/HL/NHLBI NIH HHS/United States
- F32 HL151127/HL/NHLBI NIH HHS/United States
- R01 HL154686/HL/NHLBI NIH HHS/United States
- R01 GM129312/GM/NIGMS NIH HHS/United States
- F31 AG071225/AG/NIA NIH HHS/United States
- R01 HL149883/HL/NHLBI NIH HHS/United States
- K07 CA216330/CA/NCI NIH HHS/United States
- T32 HL076139/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
