

Clinical analysis of a patient simultaneously positive for antibodies of myelin oligodendrocyte glycoprotein and anti-N-methyl-D-aspartate receptor: A case report
- PMID: 33429822
- PMCID: PMC7793424
- DOI: 10.1097/MD.0000000000024234
Clinical analysis of a patient simultaneously positive for antibodies of myelin oligodendrocyte glycoprotein and anti-N-methyl-D-aspartate receptor: A case report
Abstract
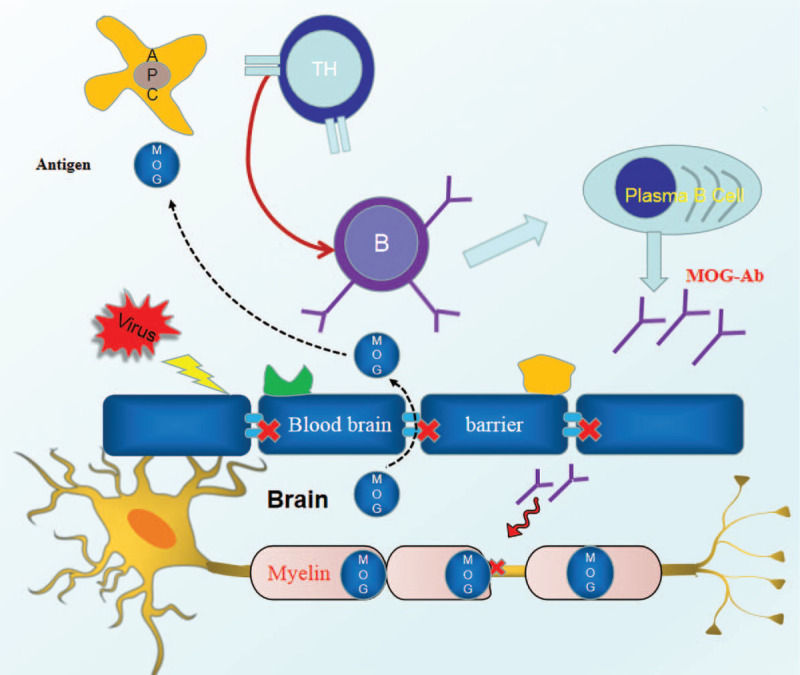
Rationale: Myelin oligodendrocyte glycoprotein (MOG) antibody (MOG-Ab) disease (MOG-AD) is a type of demyelinating disease of the central nervous system characterized by a high frequency of optic neuritis (ON) attacks. anti-Nmethyl-D-aspartate receptor (NMDAR) encephalitis (anti-NMDARe) is an autoimmune disorder characterized by memory deficits, conscious disturbance, and seizures. Cases of simultaneous occurrence of MOG-Ab and anti-NMDARe antibody (anti-NMDARe-Ab) are rarely reported and could be mistaken for overlapping MOG-antibody disease (MOG-AD) and NMDARe. The diagnosis of such patients is challenging.
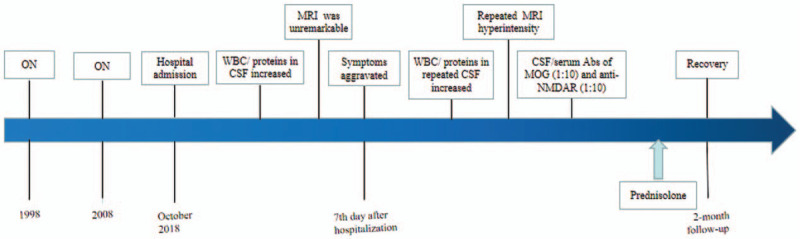
Patient concerns: We report the case of a 37-year-old man who presented with recurrent headaches for 3 months and worsening symptoms over 2 weeks. He had a history of ON. He had a generalized seizure after 7 days in the hospital.
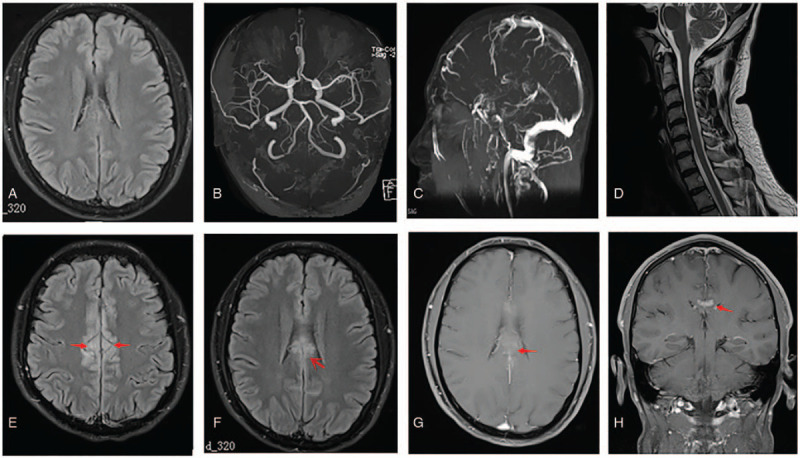
Diagnosis: Brain magnetic resonance imaging (MRI) and cerebrospinal fluid tests showed no apparent abnormalities. Repeat MRI showed slight lesions 7 days later, and cerebrospinal fluid tests showed the simultaneous occurrence of MOG-Ab and anti-NMDARe-Ab.
Interventions: He completely recovered after treatment with low doses of oral corticosteroids.
Outcomes: Two months and 2 years follow-up showed that his condition was stable.
Lessons: The co-occurrence of MOG-Ab and anti-NMDAR-Ab does not indicate the co-occurrence of MOG-AD and anti-NMDARe. Laboratory findings should be combined with the clinical features to achieve an accurate and suitable diagnosis.
Copyright © 2021 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Reindl M, Waters P. Myelin oligodendrocyte glycoprotein antibodies in neurological disease. Nat Rev Neurol 2019;15:89–102. - PubMed
-
- Bashiri FA, Al-Rasheed AA, Hassan SM, et al. Auto-immune anti-N-methyl-D-aspartate receptor (anti-NMDAR) encephalitis: three case reports. Paediatr Int Child Health 2017;37:222–6. - PubMed
-
- Ho AC, Chan SH, Chan E, et al. Anti-N-methyl-D-aspartate receptor encephalitis in children: Incidence and experience in Hong Kong. Brain Dev 2018;40:473–9. - PubMed
-
- Nagata S, Nishimura Y, Mitsuo K. A case of anti-myelin oligodendrocyte glycoprotein (MOG) and anti-N-methyl-D-aspartate (NMDA) receptor antibody-positive encephalitis with optic neuritis. Rinsho Shinkeigaku 2018;58:636–41. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
