

Immune-Checkpoint Inhibitors in B-Cell Lymphoma
- PMID: 33430146
- PMCID: PMC7827333
- DOI: 10.3390/cancers13020214
Immune-Checkpoint Inhibitors in B-Cell Lymphoma
Abstract
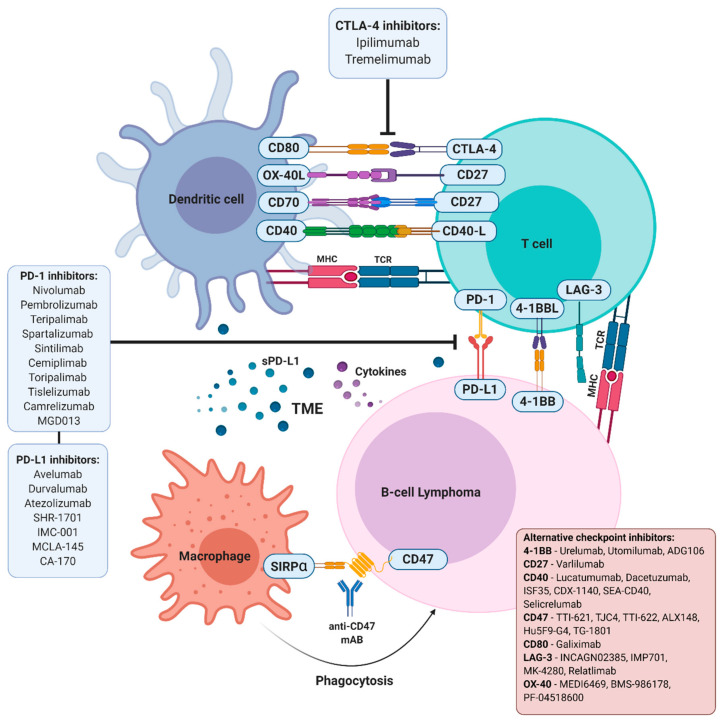
For years, immunotherapy has been considered a viable and attractive treatment option for patients with cancer. Among the immunotherapy arsenal, the targeting of intratumoral immune cells by immune-checkpoint inhibitory agents has recently revolutionised the treatment of several subtypes of tumours. These approaches, aimed at restoring an effective antitumour immunity, rapidly reached the market thanks to the simultaneous identification of inhibitory signals that dampen an effective antitumor response in a large variety of neoplastic cells and the clinical development of monoclonal antibodies targeting checkpoint receptors. Leading therapies in solid tumours are mainly focused on the cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) and programmed death 1 (PD-1) pathways. These approaches have found a promising testing ground in both Hodgkin lymphoma and non-Hodgkin lymphoma, mainly because, in these diseases, the malignant cells interact with the immune system and commonly provide signals that regulate immune function. Although several trials have already demonstrated evidence of therapeutic activity with some checkpoint inhibitors in lymphoma, many of the immunologic lessons learned from solid tumours may not directly translate to lymphoid malignancies. In this sense, the mechanisms of effective antitumor responses are different between the different lymphoma subtypes, while the reasons for this substantial difference remain partially unknown. This review will discuss the current advances of immune-checkpoint blockade therapies in B-cell lymphoma and build a projection of how the field may evolve in the near future. In particular, we will analyse the current strategies being evaluated both preclinically and clinically, with the aim of fostering the use of immune-checkpoint inhibitors in lymphoma, including combination approaches with chemotherapeutics, biological agents and/or different immunologic therapies.
Keywords: combination therapies; cytotoxic T-lymphocyte antigen 4; immune checkpoint; lymphoid neoplasms; monoclonal antibodies; programmed death 1.
Conflict of interest statement
G.R. received research support from TG Therapeutics. Remaining authors declare no conflict of interest.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
