

Combination of Cisplatin and Irradiation Induces Immunogenic Cell Death and Potentiates Postirradiation Anti-PD-1 Treatment Efficacy in Urothelial Carcinoma
- PMID: 33430352
- PMCID: PMC7825793
- DOI: 10.3390/ijms22020535
Combination of Cisplatin and Irradiation Induces Immunogenic Cell Death and Potentiates Postirradiation Anti-PD-1 Treatment Efficacy in Urothelial Carcinoma
Abstract
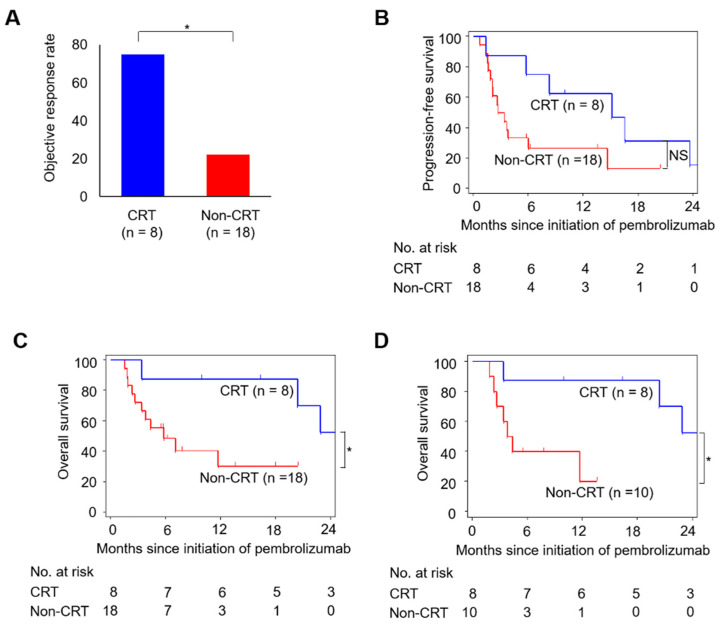
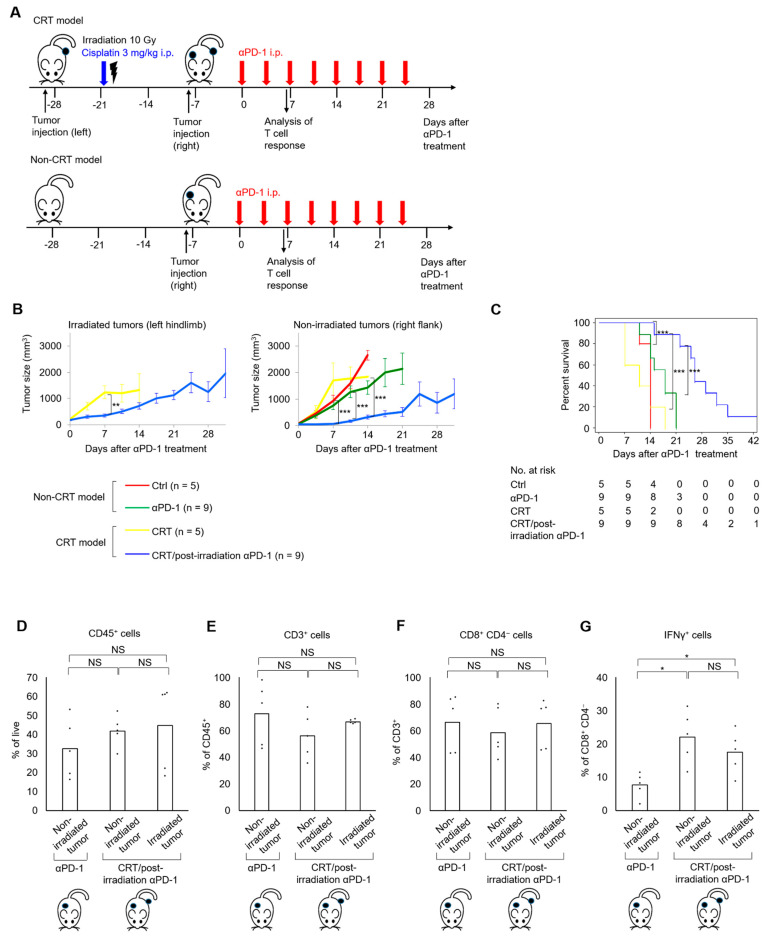
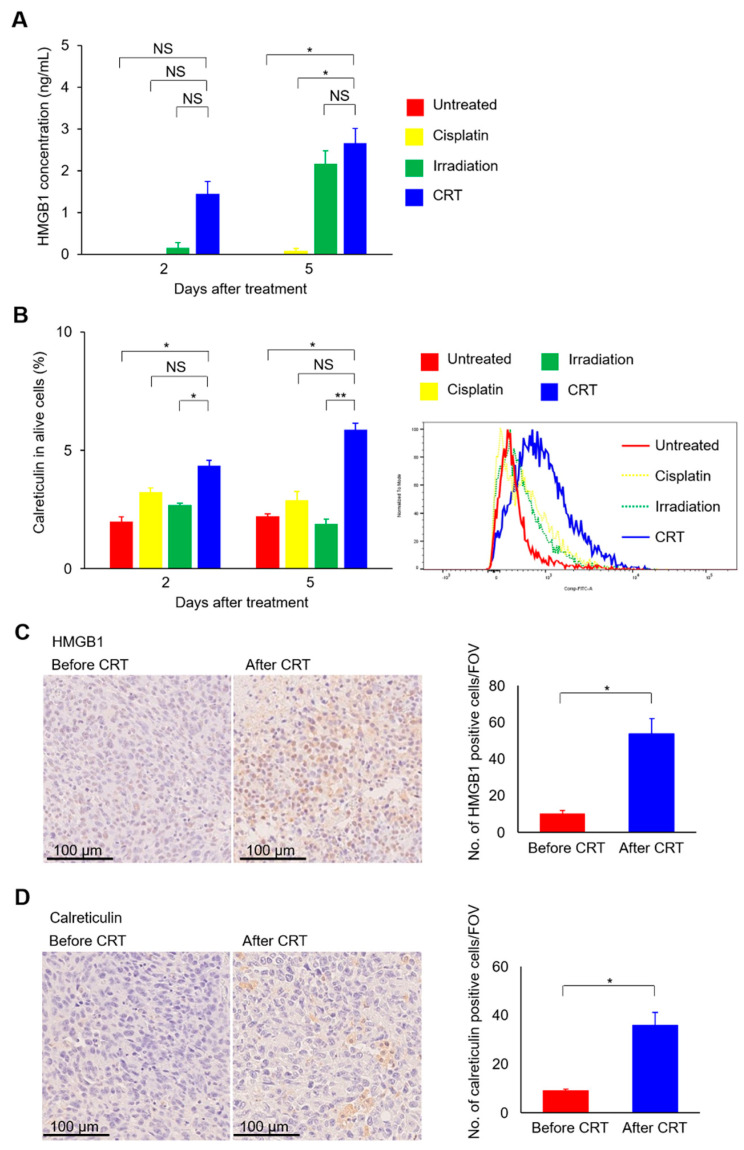
The therapeutic benefit of immune checkpoint inhibitor monotherapy is limited to a subset of patients in urothelial carcinoma (UC). Previous studies showed the immunogenicity of cisplatin and irradiation. Here, we investigated whether chemoradiotherapy (CRT), a combination of cisplatin and irradiation, could improve the efficacy of postirradiation anti-programmed cell death 1 (PD-1) treatment in UC. In our advanced UC patient cohort, patients with CRT showed a significantly better objective response rate (75%/22%) and overall survival (88%/30% at 12 months) following later pembrolizumab therapy compared to those without. Then, we created syngeneic UC mouse models by inoculating MB49 cells s.c. in C57BL/6J mice to examine the potential of CRT to enhance antitumor immunity in conjunction with postirradiation anti-PD-1 treatment. Nonirradiated tumors of the mice treated with CRT/postirradiation anti-PD-1 treatment had a significantly slower growth rate and a significantly higher expression of cytotoxic T cells compared to those of the mice treated with anti-PD-1 treatment alone. The mice treated with CRT/postirradiation anti-PD-1 treatment showed the best survival. Mechanistically, CRT provoked strong direct cytotoxicity and increased expressions of immunogenic cell death markers in MB49 cells. Therefore, the combination of cisplatin and irradiation induces immunogenic cell death and potentiates postirradiation anti-PD-1 treatment efficacy in UC.
Keywords: carcinoma; chemoradiotherapy; cisplatin; immunogenic cell death; immunotherapy; transitional cell.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures

References
-
- Bellmunt J., von der Maase H., Mead G.M., Skoneczna I., De Santis M., Daugaard G., Boehle A., Chevreau C., Paz-Ares L., Laufman L.R., et al. Randomized phase III study comparing paclitaxel/cisplatin/gemcitabine and gemcitabine/cisplatin in patients with locally advanced or metastatic urothelial cancer without prior systemic therapy: EORTC Intergroup Study 30987. J. Clin. Oncol. 2012;30:1107–1113. doi: 10.1200/JCO.2011.38.6979. - DOI - PMC - PubMed
-
- Galsky M.D., Arija J.Á.A., Bamias A., Davis I.D., De Santis M., Kikuchi E., Garcia-Del-Muro X., De Giorgi U., Mencinger M., Izumi K., et al. Atezolizumab with or without chemotherapy in metastatic urothelial cancer (IMvigor130): A multicentre, randomised, placebo-controlled phase 3 trial. Lancet. 2020;395:1547–1557. doi: 10.1016/S0140-6736(20)30230-0. - DOI - PubMed
-
- Tamura D., Jinnouchi N., Abe M., Ikarashi D., Matsuura T., Kato R., Maekawa S., Kato Y., Kanehira M., Takata R., et al. Prognostic outcomes and safety in patients treated with pembrolizumab for advanced urothelial carcinoma: Experience in real-world clinical practice. Int. J. Clin. Oncol. 2020;25:899–905. doi: 10.1007/s10147-019-01613-9. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
