

Novel MIS 3D NAV Single Step Pedicle Screw System (SSPSS): Workflow, Accuracy and Initial Clinical Experience
- PMID: 33430625
- PMCID: PMC9210221
- DOI: 10.1177/2192568220976393
Novel MIS 3D NAV Single Step Pedicle Screw System (SSPSS): Workflow, Accuracy and Initial Clinical Experience
Abstract
Study design: Prospective case series.
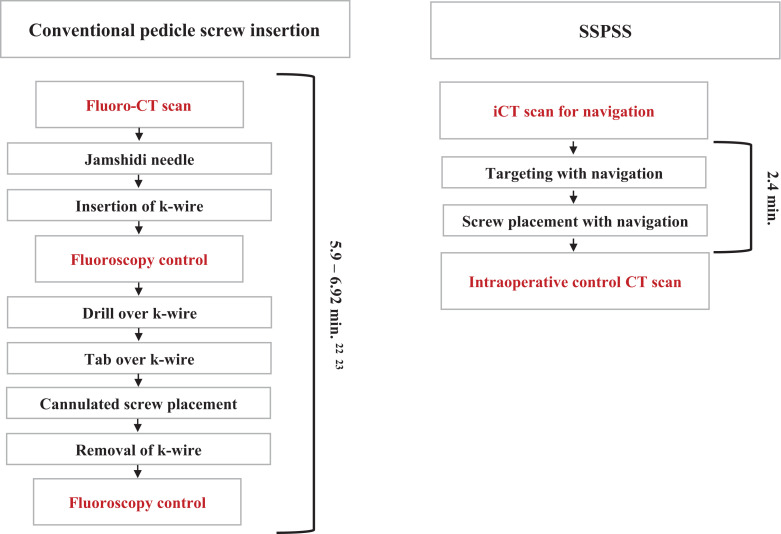
Objective: SSPSS (single step pedicle screw system) was developed for minimally invasive spine surgery. We performed this study to report on safety, workflow, and our initial clinical experience with this novel technique.
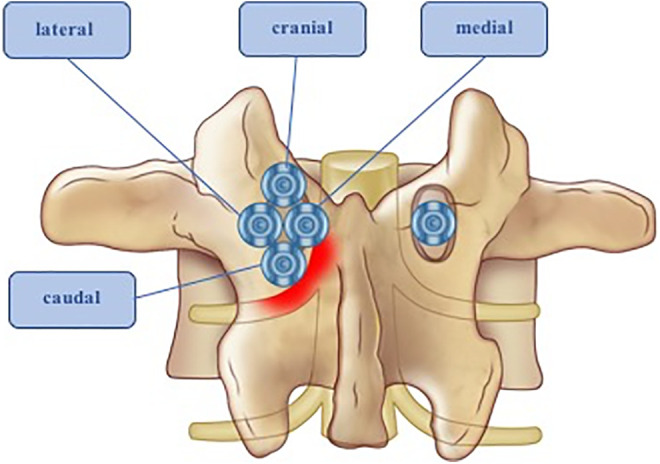
Methods: The prospective study was conducted on patients who underwent pedicle screw fixation between October 2017 and April 2018 using a novel single step 3D navigated pedicle screw system for MIS. Outcome measurements were obtained from intraoperative computerized tomography. The images were evaluated to determine pedicle wall penetration. We used a grading system to assess the severity of the pedicle wall penetration. Breaches were classified as grade 1 (<2 mm), grade 2 (2-4 mm), or grade 3 (<4 mm),1 and as cranial, caudal, medial, and lateral.
Results: Our study includes 135 screws in 24 patients. SSPSS eliminated K-wires and multiple steps traditionally necessary for MIS pedicle screw insertion. The median time per screw was 2.45 minutes. 3 screws were corrected intraoperatively. Pedicle wall penetration occurred in 14 screws (10%). Grade 1 breaches occurred in 4 screws (3%) and grade 2 breaches occurred in 10 screws (7%). Lateral breaches were observed more often than medial breaches. The accuracy rate in our study was 90% (Grade 0 breach). No revision surgeries were needed and no complications occurred.
Conclusions: Our study suggests that SSPSS could be a safe, accurate, and efficient tool. Our accuracy rate is comparable to that found in the literature.
Keywords: 3D-NAV; MIS; MISS; SSPSS; accuracy; minimally invasive; navigation; pedicle screw; screw placement; thoracolumbosacral pedicle screw system; time.
Conflict of interest statement
Figures






References
-
- Oppenheimer JH, DeCastro I, McDonnell DE. Minimally invasive spine technology and minimally invasive spine surgery: a historical review. Neurosurgical Focus. 2009;27(3):E9. - PubMed
-
- McAfee PC, Phillips FM, Andersson G, et al. Minimally invasive spine surgery. Spine. 2010;35(26 Suppl): S271–S273. - PubMed
-
- Mirza SK, Wiggins GC, Kuntz CT, et al. Accuracy of thoracic vertebral body screw placement using standard fluoroscopy, fluoroscopic image guidance, and computed tomographic image guidance: a cadaver study. Spine. 2003;28(4):402–413. - PubMed
-
- Navarro-Ramirez R, Lang G, Lian X, et al. Total navigation in spine surgery; a concise guide to eliminate fluoroscopy using a portable intraoperative computed tomography 3-dimensional navigation system. World Neurosurgery. 2017;100:325–335. - PubMed
-
- Shin BJ, Njoku IU, Tsiouris AJ, Hartl R. Navigated guide tube for the placement of mini-open pedicle screws using stereotactic 3D navigation without the use of K-wires: technical note. J Neurosurg Spine. 2013;18(2):178–183. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
