

What's the "secret sauce"? How implementation variation affects the success of colorectal cancer screening outreach
- PMID: 33431063
- PMCID: PMC7802298
- DOI: 10.1186/s43058-020-00104-7
What's the "secret sauce"? How implementation variation affects the success of colorectal cancer screening outreach
Abstract
Background: Mailed fecal immunochemical testing (FIT) programs can improve colorectal cancer (CRC) screening rates, but health systems vary how they implement (i.e., adapt) these programs for their organizations. A health insurance plan implemented a mailed FIT program (named BeneFIT), and participating health systems could adapt the program. This multi-method study explored which program adaptations might have resulted in higher screening rates.
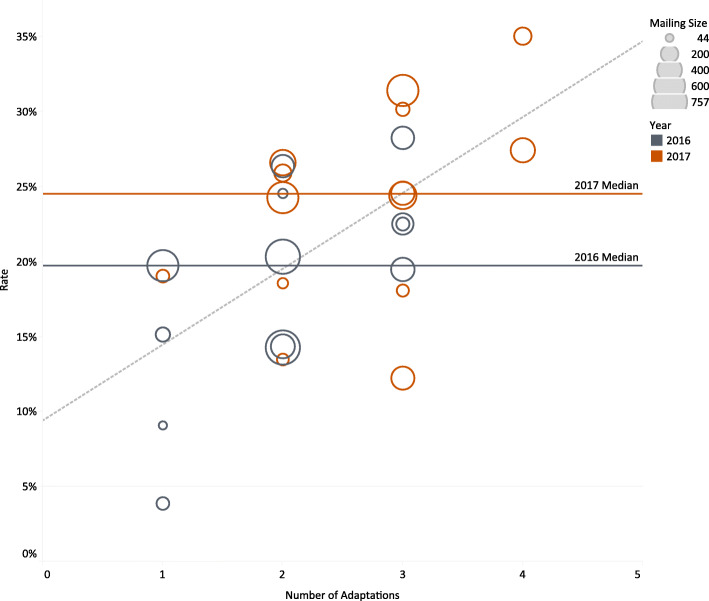
Methods: First, we conducted a descriptive analysis of CRC screening rates by key health system characteristics and program adaptations. Second, we generated an overall model by fitting a weighted regression line to our data. Third, we applied Configurational Comparative Methods (CCMs) to determine how combinations of conditions were linked to higher screening rates. The main outcome measure was CRC screening rates.
Results: Seventeen health systems took part in at least 1 year of BeneFIT. The overall screening completion rate was 20% (4-28%) in year 1 and 25% (12-35%) in year 2 of the program. Health systems that used two or more adaptations had higher screening rates, and no single adaptation clearly led to higher screening rates. In year 1, small systems, with just one clinic, that used phone reminders (n = 2) met the implementation success threshold (≥ 19% screening rate) while systems with > 1 clinic were successful when offering a patient incentive (n = 4), scrubbing mailing lists (n = 4), or allowing mailed FIT returns with no other adaptations (n = 1). In year 2, larger systems with 2-4 clinics were successful with a phone reminder (n = 4) or a patient incentive (n = 3). Of the 10 systems that implemented BeneFIT in both years, seven improved their CRC screening rates in year 2.
Conclusions: Health systems can choose among many adaptations and successfully implement a health plan's mailed FIT program. Different combinations of adaptations led to success with health system size emerging as an important contextual factor.
Keywords: Cancer prevention; Cancer screening outreach; Colorectal cancer; Implementation; Program adaptation.
Conflict of interest statement
From September 2017 to June 2018, Kaiser Permanente Center for Health Research (Dr. Coronado served as the Principal Investigator) participated in an industry-funded study to compare the clinical performance of an experimental fecal immunochemical test (FIT) to an FDA-approved FIT. This study was funded by Quidel Corporation. From February 2016 to July 2018, Jennifer Coury was contracted with CareOregon, Inc., to improve colorectal cancer screening rates in health plan members, including coordination of a mailed FIT program. All other authors declare no competing interests.
Figures
References
-
- Fedewa SA, Ma J, Sauer AG, et al. How many individuals will need to be screened to increase colorectal cancer screening prevalence to 80% by 2018? Cancer. 2015;121(23):4258–4265. - PubMed
-
- Preventive Services Task Force US, Bibbins-Domingo K, Grossman DC, et al. Screening for colorectal cancer: US Preventive Services Task Force Recommendation Statement. Jama. 2016;315(23):2564–2575. - PubMed
-
- Wilensky JD. Colorectal cancer initiatives in Medicaid agencies – a national review. Prepared for the American Cancer Society: Atlanta, GA; 2016.
-
- Centers for Medicare and Medicaid Services. Medicare Star Ratings. https://www.medicare.gov/find-a-plan/staticpages/rating/planrating-help..... Accessed 04/22/2019.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
