

Clinical and genetic differences between bipolar disorder type 1 and 2 in multiplex families
- PMID: 33431802
- PMCID: PMC7801527
- DOI: 10.1038/s41398-020-01146-0
Clinical and genetic differences between bipolar disorder type 1 and 2 in multiplex families
Abstract
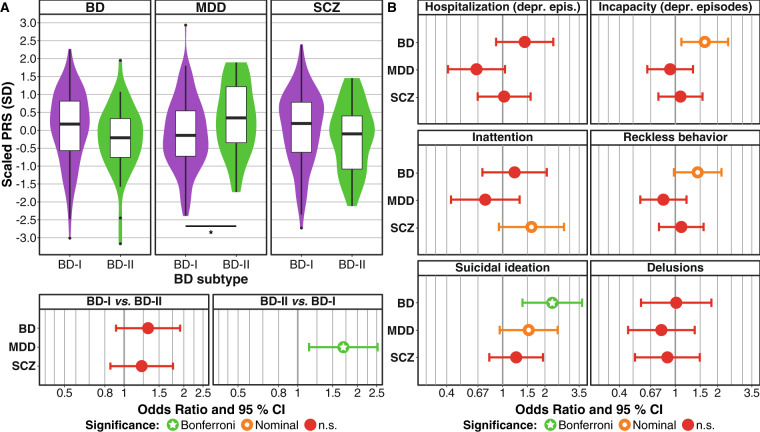
The two major subtypes of bipolar disorder (BD), BD-I and BD-II, are distinguished based on the presence of manic or hypomanic episodes. Historically, BD-II was perceived as a less severe form of BD-I. Recent research has challenged this concept of a severity continuum. Studies in large samples of unrelated patients have described clinical and genetic differences between the subtypes. Besides an increased schizophrenia polygenic risk load in BD-I, these studies also observed an increased depression risk load in BD-II patients. The present study assessed whether such clinical and genetic differences are also found in BD patients from multiplex families, which exhibit reduced genetic and environmental heterogeneity. Comparing 252 BD-I and 75 BD-II patients from the Andalusian Bipolar Family (ABiF) study, the clinical course, symptoms during depressive and manic episodes, and psychiatric comorbidities were analyzed. Furthermore, polygenic risk scores (PRS) for BD, schizophrenia, and depression were assessed. BD-I patients not only suffered from more severe symptoms during manic episodes but also more frequently showed incapacity during depressive episodes. A higher BD PRS was significantly associated with suicidal ideation. Moreover, BD-I cases exhibited lower depression PRS. In line with a severity continuum from BD-II to BD-I, our results link BD-I to a more pronounced clinical presentation in both mania and depression and indicate that the polygenic risk load of BD predisposes to more severe disorder characteristics. Nevertheless, our results suggest that the genetic risk burden for depression also shapes disorder presentation and increases the likelihood of BD-II subtype development.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- American Psychiatric Association. 5h edn (DSM-5(TM)) Arlington, VA: American Psychiatric Publishing; 2013. Diagnostic and Statistical Manual of Mental Disorders.
Publication types
MeSH terms
Grants and funding
- 01ZZ1804A (DIFUTURE)/Bundesministerium für Bildung und Forschung (Federal Ministry of Education and Research)/International
- 01ZX1314A/Bundesministerium für Bildung und Forschung (Federal Ministry of Education and Research)/International
- 01ZX1314A/Bundesministerium für Bildung und Forschung (Federal Ministry of Education and Research)/International
- 01EE1409C/Bundesministerium für Bildung und Forschung (Federal Ministry of Education and Research)/International
- 01ZX1314G/Bundesministerium für Bildung und Forschung (Federal Ministry of Education and Research)/International
- 01ZX1614G/Bundesministerium für Bildung und Forschung (Federal Ministry of Education and Research)/International
- 01EE1406C/Bundesministerium für Bildung und Forschung (Federal Ministry of Education and Research)/International
- EU RIA 733161 (MultipleMS)/EC | Horizon 2020 Framework Programme (EU Framework Programme for Research and Innovation H2020)/International
- CTS-546/Consejería de Salud, Junta de Andalucía (Ministry of Health, Andalusian Regional Government)/International
- 156791/Schweizerischer Nationalfonds zur Förderung der Wissenschaftlichen Forschung (Swiss National Science Foundation)/International
- NO246/10-2/Deutsche Forschungsgemeinschaft (German Research Foundation)/International
- RI908/11-2/Deutsche Forschungsgemeinschaft (German Research Foundation)/International
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
