

Dermatitis Herpetiformis: An Update on Diagnosis and Management
- PMID: 33432477
- PMCID: PMC8068693
- DOI: 10.1007/s40257-020-00584-2
Dermatitis Herpetiformis: An Update on Diagnosis and Management
Abstract
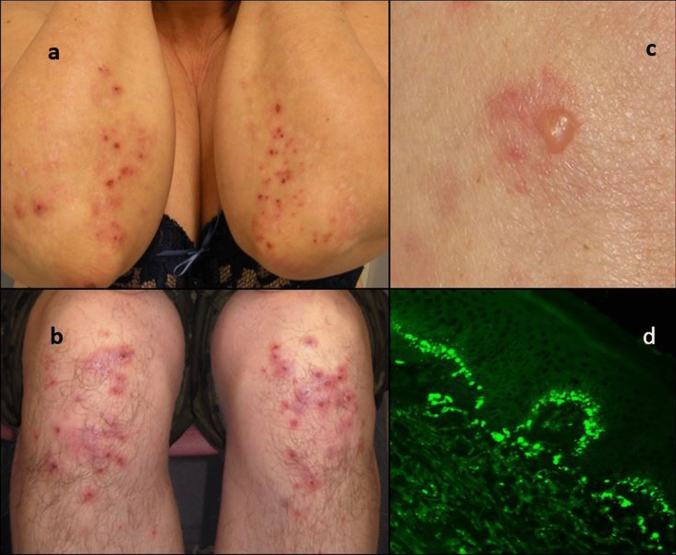
Dermatitis herpetiformis (DH), presenting with an intense itch and blistering symmetrical rash, typically on the elbows, knees, and buttocks, is a cutaneous manifestation of celiac disease. Though overt gastrointestinal symptoms are rare, three-fourths of patients with DH have villous atrophy in the small bowel, and the rest have celiac-type inflammatory changes. DH affects mostly adults and slightly more males than females. The mean age at onset is about 50 years. DH diagnosis is confirmed by showing granular immunoglobulin A deposits in the papillary dermis. The DH autoantigen, transglutaminase 3, is deposited at the same site in tightly bound immune complexes. At present, the DH-to-celiac disease prevalence is 1:8. The incidence of DH is decreasing, whereas that of celiac disease is increasing, probably because of improved diagnostics. In DH, the treatment of choice for all patients is a gluten-free diet (GFD) in which uncontaminated oats are allowed. At onset, most patients need additional dapsone to rapidly control the rash and itching. Dapsone can be stopped after a mean of 2 years, and a strict lifelong GFD alone is required. Dietary adherence offers an excellent long-term prognosis for patients with DH, with a normal quality of life and all-cause mortality.
Conflict of interest statement
Timo Reunala, Kaisa Hervonen, and Teea Salmi have no conflicts of interest that are directly relevant to the content of this article.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
