

Health Service Utilization Patterns Among Adults With Congenital Heart Disease: A Population-Based Study
- PMID: 33432841
- PMCID: PMC7955316
- DOI: 10.1161/JAHA.120.018037
Health Service Utilization Patterns Among Adults With Congenital Heart Disease: A Population-Based Study
Abstract
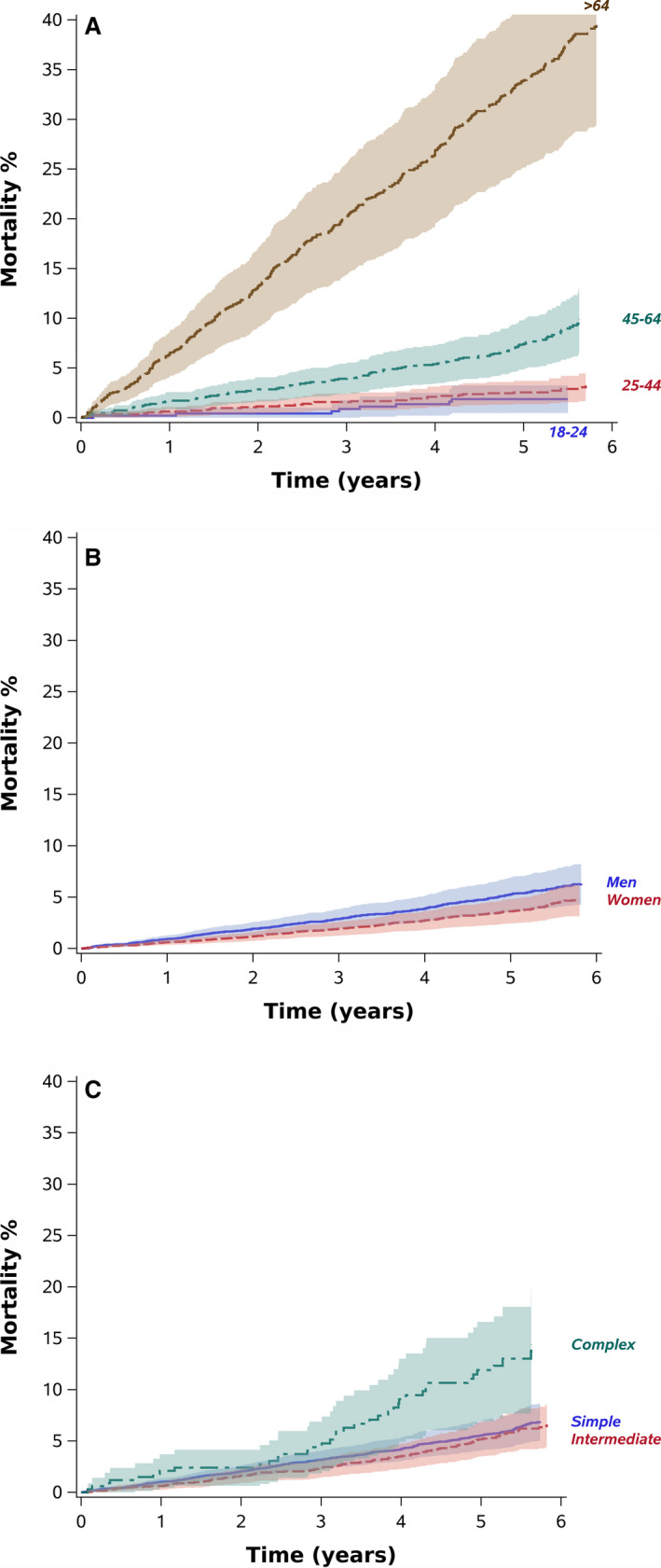
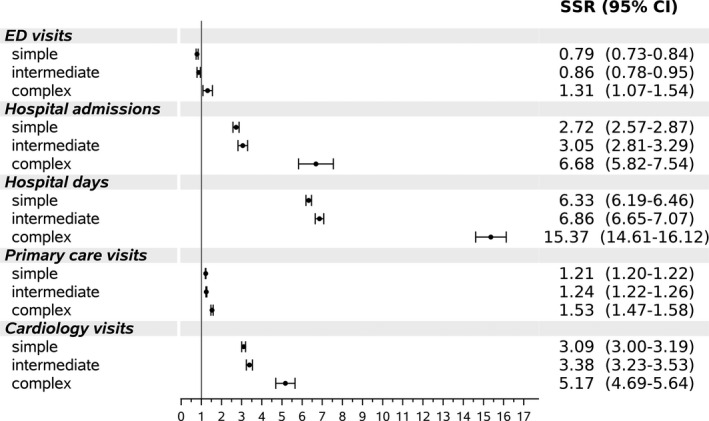
Background Several studies have examined hospitalizations among patients with adult congenital heart disease (ACHD). Few investigated other services or utilization patterns. Our aim was to study service utilization patterns and predictors among patients with ACHD. Methods and Results We identified 11 653 patients with ACHD aged ≥18 years (median, 47 years), through electronic records of 2 large Israeli healthcare providers (2007-2011). The association between patient, disease, and sociogeographic characteristics and healthcare resource utilization were modeled as recurrent events accounting for the competing death risk. Patients with ACHD had high healthcare utilization rates compared with the general population. The highest standardized service utilization ratios (SSRs) were found among patients with complex congenital heart disease including primary care visits (SSR, 1.53; 95% CI, 1.47-1.58), cardiology outpatient visits (SSR, 5.17; 95% CI, 4.69-5.64), hospitalizations (SSR, 6.68; 95% CI, 5.82-7.54), and days in hospital (SSR, 15.37; 95% CI, 14.61-16.12). Adjusted resource utilization hazard increased with increasing lesion complexity. Hazard ratios (HRs) for complex versus simple disease were: primary care (HR, 1.14; 95% CI, 1.06-1.23); cardiology outpatient visits (HR, 1.40; 95% CI, 1.24-1.59); emergency department visits (HR, 1.19; 95% CI, 1.02-1.39); and hospitalizations (HR, 1.75; 95% CI, 1.49-2.05). Effects attenuated with age for cardiology outpatient visits and hospitalizations and increased for emergency department visits. Female sex, geographic periphery, and ethnic minority were associated with more primary care visits, and female sex (HR versus men, 0.89 [95% CI, 0.84-0.94]) and periphery (HR, 0.72 [95% CI, 0.58-0.90] for very peripheral versus very central) were associated with fewer cardiology visits. Arab minority patients also had high hospitalization rates compared with the majority group of Jewish or other patients. Conclusions Healthcare utilization rates were high among patients with ACHD. Female sex, geographic periphery, and ethnicity were associated with less optimal service utilization patterns. Further research should examine strategies to optimize service utilization in these groups.
Keywords: adult congenital heart disease; healthcare service utilization; mortality; population‐based study.
Conflict of interest statement
None.
Figures
References
-
- Baumgartner H, Bonhoeffer P, De Groot NM, de Haan F, Deanfield JE, Galie N, Gatzoulis MA, Gohlke‐Baerwolf C, Kaemmerer H, Kilner P, et al. Task Force on the management of grown‐up congenital heart disease of the European Society of Cardiology (ESC); Association for European Paediatric Cardiology (AEPC); ESC Committee for Practice Guidelines (CPG). ESC guidelines for the management of grown‐up congenital heart disease (new version 2010). Eur Heart J. 2010;31:2915–2957. - PubMed
-
- Webb G, Mulder BJ, Aboulhosn J, Daniels CJ, Elizari MA, Hong GU, Horlick E, Landzberg MJ, Marelli AJ, O'Donnell CP, et al. The care of adults with congenital heart disease across the globe: current assessment and future perspective: a position statement from the International Society for Adult Congenital Heart Disease (ISACHD). Int J Cardiol. 2015;195:326–333. DOI: 10.1016/j.ijcard.2015.04.230 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
