

Epidemiological Characteristics, Ventilator Management, and Clinical Outcome in Patients Receiving Invasive Ventilation in Intensive Care Units from 10 Asian Middle-Income Countries (PRoVENT-iMiC): An International, Multicenter, Prospective Study
- PMID: 33432906
- PMCID: PMC7941813
- DOI: 10.4269/ajtmh.20-1177
Epidemiological Characteristics, Ventilator Management, and Clinical Outcome in Patients Receiving Invasive Ventilation in Intensive Care Units from 10 Asian Middle-Income Countries (PRoVENT-iMiC): An International, Multicenter, Prospective Study
Abstract
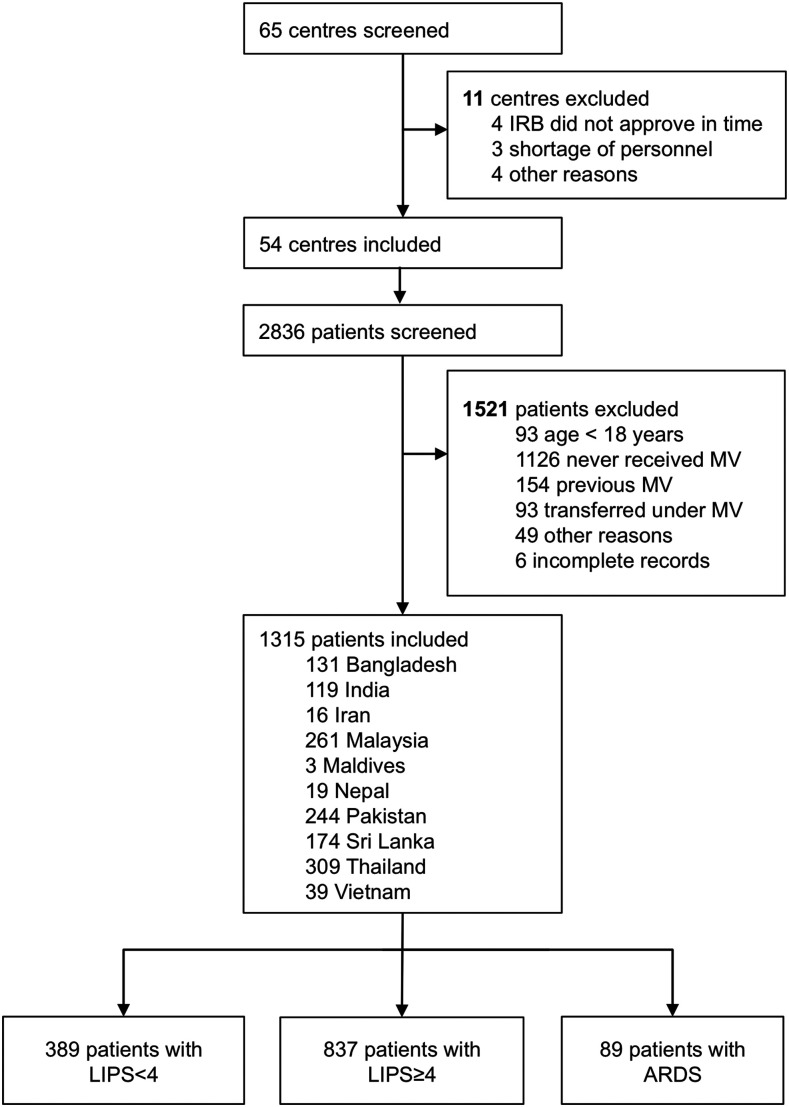
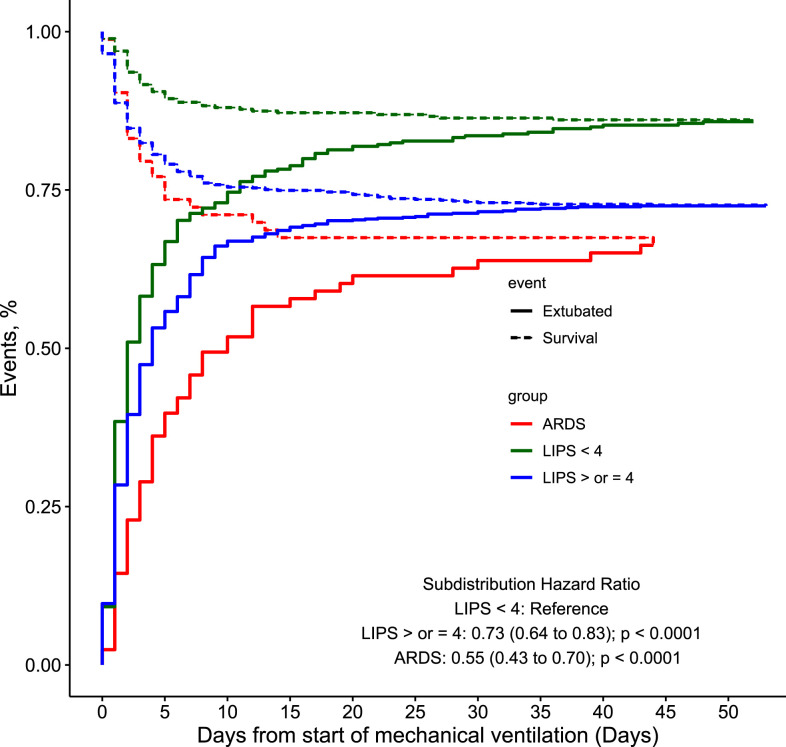
Epidemiology, ventilator management, and outcome in patients receiving invasive ventilation in intensive care units (ICUs) in middle-income countries are largely unknown. PRactice of VENTilation in Middle-income Countries is an international multicenter 4-week observational study of invasively ventilated adult patients in 54 ICUs from 10 Asian countries conducted in 2017/18. Study outcomes included major ventilator settings (including tidal volume [V T ] and positive end-expiratory pressure [PEEP]); the proportion of patients at risk for acute respiratory distress syndrome (ARDS), according to the lung injury prediction score (LIPS), or with ARDS; the incidence of pulmonary complications; and ICU mortality. In 1,315 patients included, median V T was similar in patients with LIPS < 4 and patients with LIPS ≥ 4, but lower in patients with ARDS (7.90 [6.8-8.9], 8.0 [6.8-9.2], and 7.0 [5.8-8.4] mL/kg Predicted body weight; P = 0.0001). Median PEEP was similar in patients with LIPS < 4 and LIPS ≥ 4, but higher in patients with ARDS (five [5-7], five [5-8], and 10 [5-12] cmH2O; P < 0.0001). The proportions of patients with LIPS ≥ 4 or with ARDS were 68% (95% CI: 66-71) and 7% (95% CI: 6-8), respectively. Pulmonary complications increased stepwise from patients with LIPS < 4 to patients with LIPS ≥ 4 and patients with ARDS (19%, 21%, and 38% respectively; P = 0.0002), with a similar trend in ICU mortality (17%, 34%, and 45% respectively; P < 0.0001). The capacity of the LIPS to predict development of ARDS was poor (receiver operating characteristic [ROC] area under the curve [AUC] of 0.62, 95% CI: 0.54-0.70). In Asian middle-income countries, where two-thirds of ventilated patients are at risk for ARDS according to the LIPS and pulmonary complications are frequent, setting of V T is globally in line with current recommendations.
Conflict of interest statement
Members of the PRoVENT-iMiC Steering Committee: Luigi Pisani (Mahidol-Oxford Tropical Medicine Research Unit, Bangkok, Thailand; Amsterdam University Medical Centers, Location AMC, Amsterdam, The Netherlands); Ary Serpa Neto (Amsterdam University Medical Centers, Location AMC, Amsterdam, The Netherlands; Hospital Israelita Albert Einstein, São Paulo, Brazil); Anna Geke Algera (Amsterdam University Medical Centers, Location AMC, Amsterdam, The Netherlands); Salvatore Grasso (Bari University Policlinic Hospital, University of Bari, Bari, Italy); Frederique Paulus (Amsterdam University Medical Centers, Location AMC, Amsterdam, The Netherlands); Marcelo Gama de Abreu (University Hospital Carl Gustav Carus, and Technical University Dresden, Dresden, Germany); Paolo Pelosi (San Martino Policlinico Hospital - IRCCS for Oncology, University of Genoa, Genoa, Italy); Arjen M. Dondorp (Mahidol University, Bangkok, Thailand); Marcus J. Schultz (Mahidol-Oxford Tropical Medicine Research Unit, Bangkok, Thailand; Amsterdam University Medical Centers, Location AMC, Amsterdam, The Netherlands; University of Oxford, Oxford, United Kingdom).
Members of the PRoVENT-iMiC Writing Committee: Luigi Pisani (Mahidol–Oxford Tropical Medicine Research Unit, Bangkok, Thailand; Amsterdam University Medical Centers, Location AMC, Amsterdam, The Netherlands); Ary Serpa Neto (Hospital Israelita Albert Einstein, São Paulo, Brazil; and Faculdade de Medicina do ABC, Santo André, Brazil); Arjen M. Dondorp (Mahidol–Oxford Tropical Medicine Research Unit, Bangkok, Thailand); Marcus J. Schultz (Mahidol–Oxford Tropical Medicine Research Unit, Bangkok, Thailand; Amsterdam University Medical Centers, Location AMC, Amsterdam, The Netherlands, University of Oxford, Oxford, United Kingdom).
PRactice of VENTilation in Middle-income Countries collaborators by COUNTRY (in alphabetical order)
BANGLADESH: AKM Shamsul Alam, Syeda Nafisa Khatoon, Ranjan Kumer Nath, Mohammed Abdur Rahman Chowdhury (Chittagong Medical College Hospital, Chittagong, Bangladesh); Debabrata Banik, Montosh Kumar Mondol, Sakibur Rahman Bhuiyan (Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh); Areef Ahsan, Suraiya Nazneen, Rozina Sultana, Tarikul Hamid (BIRDEM General Hospital, Dhaka, Bangladesh); Mozaffer Hossain, Syed Tariq Reza, Muhammad Asaduzzaman, Mohammad Salim, (Dhaka Medical College Hospital, Dhaka, Bangladesh); Abu Hena Mostafa Kamal, Sheikh Mohammed Taher, Taohidul Majid Taohid, Pranab Karmaker (Rajshahi Medical College Hospital, Rajshahi, Bangladesh); Sabyasachi Roy, Shantanu Das, Sohel Ahmed Sarkar, Monju Lal Dutta, Poulomi Roy (Sylhet MAG Osmani Medical College Hospital, Sylhet, Bangladesh) – INDIA: Bhuvana Krishna, Sriram Sampath (St. John’s Medical College, Bangalore); Chinni Krishna Kasi, Rajyabardhan Pattnaik, (Ispat General Hospital, Rourkela, India); Shiva Iyer, Jignesh Shah (Bharati Vidyapeeth Medical College, Pune, India); Anand Dongre (Swastik Critical Care, Nagpur, India) – IRAN: Navid Nooraei (Modarres Hospital, Tehran, Iran); Reza Hashemian, Reza Raessi Estabragh, Majid Malekmohammad (Masih Daneshvari Hospital, Tehran, Iran); Batoul Khoundabi (Red Crescent Society of the Islamic Republic of Iran, Tehran, Iran); Maziar Mobasher (Tehran Pars Hospital, Tehran, Iran) – MALAYSIA: Nor’azim Mohd Yunos, Mahazir Kassim, Voon Chern Min, Stanis Sutharsa Das, Siti Nur Suhaila Azauddin, Dharshinie Dorasamy, (Hospital Sultanah Aminah Johor Bahru, Malaysia); Tai Li Ling (Hospital Kuala Lumpur, Kuala Lumpur, Malaysia); Mohd Basri Mat Nor, Nurhafizah Zarudin (International Islamic University Medical Centre, Kuantan, Malaysia); Mohd Shahnaz Hassan, Mohamad Fadhil Hadi Jamaluddin, Mohamad Irfan Bin Othman Jailani, (University of Malaya Medical Centre, Kuala Lumpur, Malaysia) – MALDIVES: Hassan Moosa, Hisham Ahmed Imad (Indira Gandhi Memorial Hospital, Malé, Maldives) – NEPAL: Gyan Kayastha, Aaradhana Adhikari, Raju Pangeni (Patan Academy of Health Sciences, Kathmandu, Nepal) – PAKISTAN: Sonia Joseph (Allied Hospital, Faisalabad, Pakistan); Aftab Akhtar, Aayesha Qadeer (Shifa International Hospital, Islamabad, Pakistan); Iqbal Memon, Syed Muneeb Ali (Pakistan Institute of Medical Sciences, Islamabad, Pakistan); Farah Idrees, Saima Kamal (Aga Khan University, Karachi, Pakistan); Sadaf Hanif, Atta Ur Rehman (Patel Hospital, Karachi, Pakistan); Arshad Taqi, Tanveer Hussain (National Hospital and Medical Center, Lahore, Pakistan); Ahmed Farooq (Doctor’s Hospital, Lahore, Pakistan); Saleh Khaskheli (Peoples Medical College Hospital, Nawabshah, Pakistan); Muhammad Hayat (North West General Hospital, Peshawar, Pakistan) – SRI LANKA: Upeka Samaranayake (Anuradhapura Teaching Hospital, Anuradhapura, Sri Lanka); S. Mathanalagan (Base Hospital, Batticaloa, Sri Lanka); Asoka Gunaratne (Colombo South Teaching Hospital, Colombo, Sri Lanka); Kanishka Indraratna, Nimangee Mithraratne, Kaushila Thilakasiri, Chamila Pilimatalawwe, Y. A. Hasitha Dilhani (General Hospital Sri Jayawardenapura, Colombo, Sri Lanka); Marie Fernando, Kumudini Ranatunge (National Hospital Sri Lanka – SICU, Colombo, Sri Lanka); Loranthi Samarasinghe, Manori Vaas (Lanka Hospital, Colombo, Sri Lanka); Manoj Edirisooriya (National Hospital Sri Lanka – MICU, Colombo, Sri Lanka); Chaturani Sigera (Network for improving Critical Care Systems and Training, Colombo, Sri Lanka); Janaki Arumoli (Jaffna Teaching Hospital, Jaffna, Sri Lanka); Kesharie De Silva (Karapitiya Teaching Hospital, Galle, Sri Lanka); Bimal Kudavidanage (Base Hospital, Kegalle, Sri Lanka); Visanthi Pinto (Peradenyia University Hospital, Peradenyia, Sri Lanka); Lakshman Dissanayake (Puttalam Base Hospital, Puttalam, Sri Lanka) – THAILAND: Napplika Kongpolprom (King Chulalongkorn Memorial Hospital, Chulalongkorn University, Bankgok, Thailand); Hisham Ahmed, Udomsak Silachamroon (Hospital for Tropical Diseases, Mahidol University, Bangkok, Thailand); Prapaporn Pornsuriyasak, Tananchai Petnak, Pongsasit Singhatas, Viratch Tangsujaritvijit (Ramathibodi Hospital, Bangkok, Thailand); Suthat Rungruanghiranya (Srinakharinwirot University, Ongkarak, Thailand); Annop Piriyapatsom (Sriraj Hospital, Bankok, Thailand); Kaweesak Chittawatanarat, Kanokkarn Juntaping (SICU, Department of Surgery, Faculty of Medicine, Chiang Mai University, Maharaj Nakorn Chiang Mai Hospital, Chiang Mai, Thailand); Konlawij Trongtrakul, Poungrat Thungtitikul (Vajira Hospital, Bangkok, Thailand); Pattraporn Tajarernmuang (Chiang Mai Hospital – MICU, Chiang Mai, Thailand); Sunisa Chatmongkolchart, Rungsun Bhurayanontachai, Osaree Akaraborworn, Asma Navasakulpong (Prince of Songkla University, Hatyai, Thailand); Karjbundid Surasit (Nakornping Hospital, Chiang Mai, Thailand); – VIET NAM: Behzad Nadjm, Vu Quoc Dat, Nguyen Thi Thanh Ha, Nguyen Van Kinh (National Hospital for Tropical Diseases, Hanoi, Viet Nam); Duong Bich Thuy (Hospital for Tropical Diseases, Ho Chi Minh City, Vietnam); Lam Minh Yen, Louise Thwaites (Oxford University Clinical Research Unit, Ho Chi Minh City, Viet Nam).
Financial support: External funding source for this study was sought only in Vietnam (Wellcome Trust Grants 107367/Z/15/Z and 089276/B/09/7).
Disclosure: The members of the PRoVENT-iMiC Steering Committee and the national coordinators designed and overviewed the conduct of the study. PRoVENT-iMiC collaborators, consisting of national coordinators and local investigators, collected the data. This study report was written by the members of the PRoVENT-iMiC Writing Committee and revised by the PRoVENT-iMiC Steering Committee and all National Coordinators. L. P. and A. S. N. had complete access to all study data and performed the analyses, with support from A. M. D. and M. J. S. L. P., A. S. N., A. M. D., and M. J. S. made the final decision to submit the report for publication. L. P. was the study coordinator. L. P. and A. S. N. contributed equally to this study.
Figures


References
-
- Slutsky AS, Ranieri VM, 2014. Ventilator-induced lung injury. N Engl J Med 370: 980. - PubMed
-
- Esteban A, et al. 2002. Characteristics and outcomes in adult patients receiving mechanical ventilation: a 28-day international study. JAMA 287: 345–355. - PubMed
-
- Esteban A, et al. 2008. Evolution of mechanical ventilation in response to clinical research. Am J Respir Crit Care Med 177: 170–177. - PubMed
-
- Esteban A, et al. 2013. Evolution of mortality over time in patients receiving mechanical ventilation. Am J Respir Crit Care Med 188: 220–230. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
