

Pharmacologic Management of Intensive Care Unit Delirium: Clinical Prescribing Practices and Outcomes in More Than 8500 Patient Encounters
- PMID: 33433117
- PMCID: PMC8793637
- DOI: 10.1213/ANE.0000000000005365
Pharmacologic Management of Intensive Care Unit Delirium: Clinical Prescribing Practices and Outcomes in More Than 8500 Patient Encounters
Abstract
Background: Pharmacologic agents are frequently utilized for management of intensive care unit (ICU) delirium, yet prescribing patterns and impact of medication choices on patient outcomes are poorly described. We sought to describe prescribing practices for management of ICU delirium and investigate the independent association of medication choice on key in-hospital outcomes including delirium resolution, in-hospital mortality, and days alive and free of the ICU or hospital.
Methods: A retrospective study of delirious adult ICU patients at a tertiary academic medical center. Data were obtained regarding daily mental status (normal, delirious, and comatose), pharmacologic treatment, hospital course, and survival via electronic health record. Daily transition models were constructed to assess the independent association of previous day mental status and medication administration on mental status the following day and in-hospital mortality, after adjusting for prespecified covariates. Linear regression models investigated the association of medication administration on days alive and free of the ICU or the hospital during the first 30 days after ICU admission.
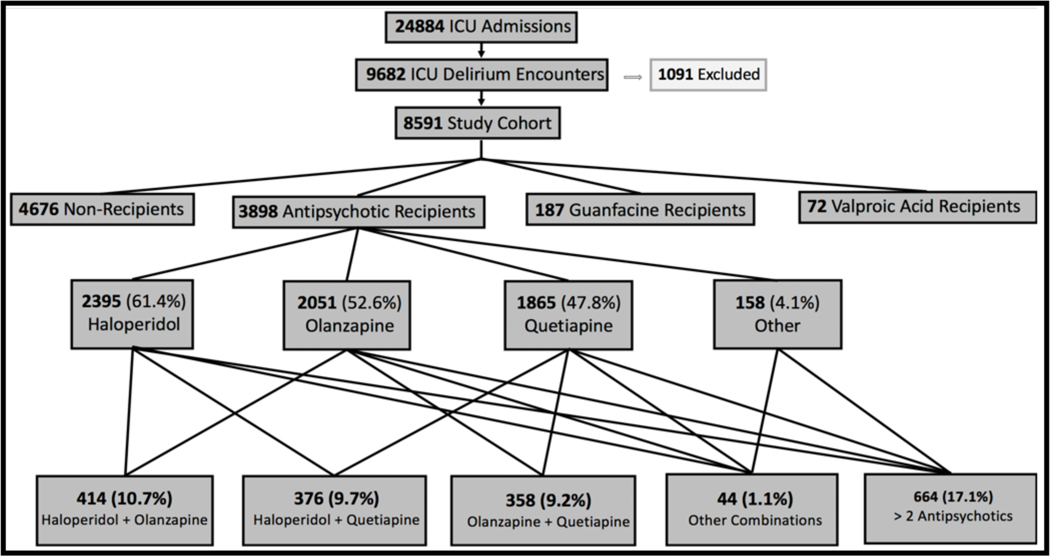
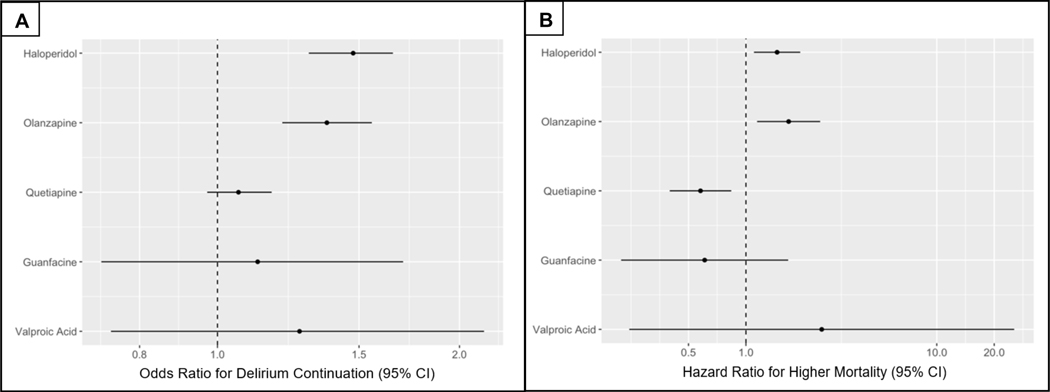
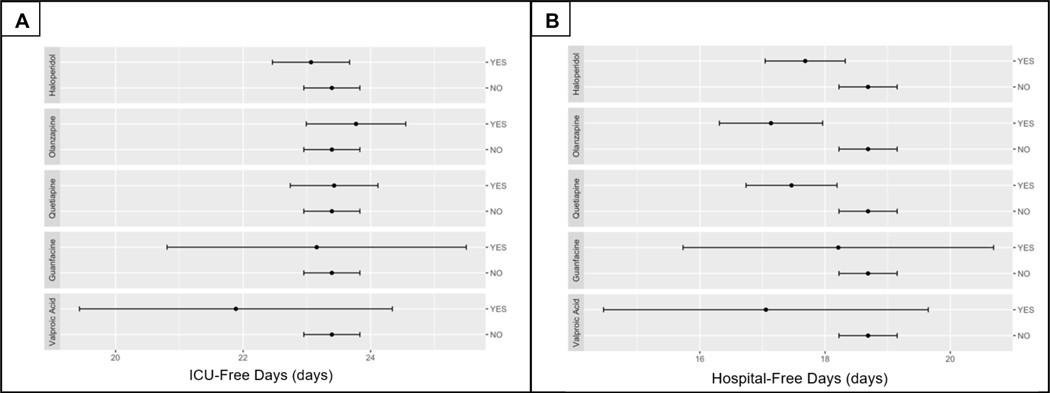
Results: We identified 8591 encounters of ICU delirium. Half (45.6%) of patients received pharmacologic treatment for delirium, including 45.4% receiving antipsychotics, 2.2% guanfacine, and 0.84% valproic acid. Median highest Richmond Agitation-Sedation Scale (RASS) score was 1 (0, 1) in patients initiated on medications and 0 (-1, 0) for nonrecipients. Haloperidol, olanzapine, and quetiapine comprised >97% of antipsychotics utilized with 48% receiving 2 or more and 20.6% continued on antipsychotic medications at hospital discharge. Haloperidol and olanzapine were associated with greater odds of continued delirium (odds ratio [OR], 1.48; 95% confidence interval [95% CI], 1.30-1.65; P < .001 and OR, 1.37; 95% CI, 1.20-1.56; P = .003, respectively) and increased hazard of in-hospital mortality (hazard ratio [HR], 1.46; 95% CI, 1.10-1.93; P = .01 and HR, 1.67; 95% CI, 1.14-2.45; P = .01, respectively) while quetiapine showed a decreased hazard of in-hospital mortality (HR, 0.58; 95% CI, 0.40-0.84; P = .01). Haloperidol, olanzapine, and quetiapine were associated with fewer days alive and free of hospitalization (all P < .001). There was no significant association of any antipsychotic medication with days alive and free of the ICU. Neither guanfacine nor valproic acid were associated with in-hospital outcomes examined.
Conclusions: Pharmacologic interventions for management of ICU delirium are common, most often with antipsychotics, and frequently continued at hospital discharge. These medications may not portend benefit, may introduce additional harm, and should be used with caution for delirium management. Continuation of these medications through hospitalization and discharge draws into question their safety and role in patient recovery.
Copyright © 2021 International Anesthesia Research Society.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Association AP: Diagnostic and statistical manual of mental disorders, fifth edition. Washington, DC., American Psychiatric Association, 2013
-
- Ouimet S, Kavanagh BP, Gottfried SB, Skrobik Y. Incidence, risk factors and consequences of ICU delirium. Intensive Care Med. 2007;33(1):66–73. - PubMed
-
- Ely EW, Shintani A, Truman B, et al. Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. Jama. 2004;291(14):1753–1762. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
