

Effect of Out-of-Hospital Sodium Nitrite on Survival to Hospital Admission After Cardiac Arrest: A Randomized Clinical Trial
- PMID: 33433575
- PMCID: PMC7804921
- DOI: 10.1001/jama.2020.24326
Effect of Out-of-Hospital Sodium Nitrite on Survival to Hospital Admission After Cardiac Arrest: A Randomized Clinical Trial
Abstract
Importance: Therapeutic delivery of sodium nitrite during resuscitation improved survival in animal models of cardiac arrest, but efficacy has not been evaluated in clinical trials in humans.
Objective: To determine whether parenteral administration of sodium nitrite given by paramedics during resuscitation for out-of-hospital cardiac arrest improved survival to hospital admission.
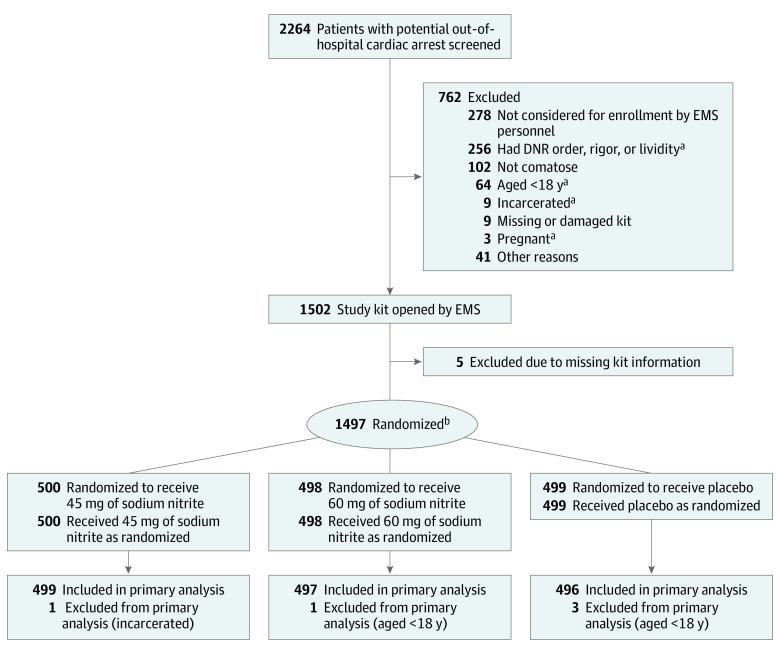
Design, setting, and participants: Double-blind, placebo-controlled, phase 2 randomized clinical trial including 1502 adults in King County, Washington, with out-of-hospital cardiac arrest from ventricular fibrillation or nonventricular fibrillation. Patients underwent resuscitation by paramedics and were enrolled between February 8, 2018, and August 19, 2019; follow-up and data abstraction were completed by December 31, 2019.
Interventions: Eligible patients with out-of-hospital cardiac arrest were randomized (1:1:1) to receive 45 mg of sodium nitrite (n = 500), 60 mg of sodium nitrite (n = 498), or placebo (n = 499), which was given via bolus injection by the paramedics as soon as possible during active resuscitation.
Main outcomes and measures: The primary outcome was survival to hospital admission and was evaluated with 1-sided hypothesis testing. The secondary outcomes included out-of-hospital variables (rate of return of spontaneous circulation, rate of rearrest, and use of norepinephrine to support blood pressure) and in-hospital variables (survival to hospital discharge; neurological outcomes at hospital discharge; cumulative survival to 24 hours, 48 hours, and 72 hours; and number of days in the intensive care unit).
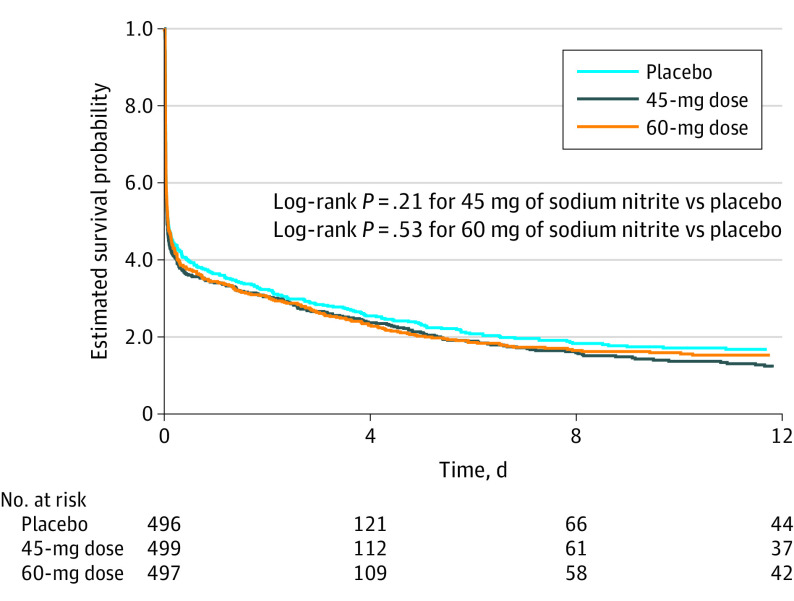
Results: Among 1502 patients with out-of-hospital cardiac arrest who were randomized (mean age, 64 years [SD, 17 years]; 34% were women), 99% completed the trial. Overall, 205 patients (41%) in the 45 mg of sodium nitrite group and 212 patients (43%) in the 60 mg of sodium nitrite group compared with 218 patients (44%) in the placebo group survived to hospital admission; the mean difference for the 45-mg dose vs placebo was -2.9% (1-sided 95% CI, -8.0% to ∞; P = .82) and the mean difference for the 60-mg dose vs placebo was -1.3% (1-sided 95% CI, -6.5% to ∞; P = .66). None of the 7 prespecified secondary outcomes were significantly different, including survival to hospital discharge for 66 patients (13.2%) in the 45 mg of sodium nitrite group and 72 patients (14.5%) in the 60 mg of sodium nitrite group compared with 74 patients (14.9%) in the placebo group; the mean difference for the 45-mg dose vs placebo was -1.7% (2-sided 95% CI, -6.0% to 2.6%; P = .44) and the mean difference for the 60-mg dose vs placebo was -0.4% (2-sided 95% CI, -4.9% to 4.0%; P = .85).
Conclusions and relevance: Among patients with out-of-hospital cardiac arrest, administration of sodium nitrite, compared with placebo, did not significantly improve survival to hospital admission. These findings do not support the use of sodium nitrite during resuscitation from out-of-hospital cardiac arrest.
Trial registration: ClinicalTrials.gov Identifier: NCT03452917.
Conflict of interest statement
Figures
Comment in
-
Effect of Sodium Nitrite on Survival of Cardiac Arrest to Hospital Admission.JAMA. 2021 May 25;325(20):2118. doi: 10.1001/jama.2021.4064. JAMA. 2021. PMID: 34032838 No abstract available.
Similar articles
-
Effect of Lower vs Higher Oxygen Saturation Targets on Survival to Hospital Discharge Among Patients Resuscitated After Out-of-Hospital Cardiac Arrest: The EXACT Randomized Clinical Trial.JAMA. 2022 Nov 8;328(18):1818-1826. doi: 10.1001/jama.2022.17701. JAMA. 2022. PMID: 36286192 Free PMC article.
-
Usefulness of Intravenous Sodium Nitrite During Resuscitation for the Treatment of Out-of-Hospital Cardiac Arrest.Am J Cardiol. 2018 Aug 15;122(4):554-559. doi: 10.1016/j.amjcard.2018.04.060. Epub 2018 Jun 20. Am J Cardiol. 2018. PMID: 30205886 Free PMC article.
-
Effect of prehospital induction of mild hypothermia on survival and neurological status among adults with cardiac arrest: a randomized clinical trial.JAMA. 2014 Jan 1;311(1):45-52. doi: 10.1001/jama.2013.282173. JAMA. 2014. PMID: 24240712 Clinical Trial.
-
Epinephrine for Out-of-Hospital Cardiac Arrest: An Updated Systematic Review and Meta-Analysis.Crit Care Med. 2020 Feb;48(2):225-229. doi: 10.1097/CCM.0000000000004130. Crit Care Med. 2020. PMID: 31939791
-
The global survival rate among adult out-of-hospital cardiac arrest patients who received cardiopulmonary resuscitation: a systematic review and meta-analysis.Crit Care. 2020 Feb 22;24(1):61. doi: 10.1186/s13054-020-2773-2. Crit Care. 2020. PMID: 32087741 Free PMC article.
Cited by
-
Effects of Sodium Nitroprusside Administered Via a Subdural Intracranial Catheter on the Microcirculation, Oxygenation, and Electrocortical Activity of the Cerebral Cortex in a Pig Cardiac Arrest Model.J Am Heart Assoc. 2022 Jun 7;11(11):e025400. doi: 10.1161/JAHA.122.025400. Epub 2022 May 27. J Am Heart Assoc. 2022. PMID: 35624079 Free PMC article.
-
Temporal Patterns in Out-of-Hospital Cardiac Arrest Incidence and Outcome.JAMA Cardiol. 2025 Jul 16:e252247. doi: 10.1001/jamacardio.2025.2247. Online ahead of print. JAMA Cardiol. 2025. PMID: 40668576 Free PMC article.
-
Nitrate Metabolism and Ischemic Cerebrovascular Disease: A Narrative Review.Front Neurol. 2022 Mar 3;13:735181. doi: 10.3389/fneur.2022.735181. eCollection 2022. Front Neurol. 2022. PMID: 35309590 Free PMC article. Review.
-
Trend of Outcome Metrics in Recent Out-of-Hospital-Cardiac-Arrest Research: A Narrative Review of Clinical Trials.J Clin Med. 2023 Nov 20;12(22):7196. doi: 10.3390/jcm12227196. J Clin Med. 2023. PMID: 38002808 Free PMC article. Review.
-
Latest in Resuscitation Research: Highlights From the 2021 American Heart Association's Resuscitation Science Symposium.J Am Heart Assoc. 2022 Oct 4;11(19):e026191. doi: 10.1161/JAHA.122.026191. Epub 2022 Sep 29. J Am Heart Assoc. 2022. PMID: 36172932 Free PMC article. No abstract available.
References
-
- Panchal AR, Berg KM, Cabañas JG, et al. . 2019 American Heart Association focused update on systems of care. Circulation. 2019;140(24):e895-e903. - PubMed
-
- Neumar RW, Nolan JP, Adrie C, et al. . Post-cardiac arrest syndrome: epidemiology, pathophysiology, treatment, and prognostication. Circulation. 2008;118(23):2452-2483. - PubMed
-
- Callaway CW, Soar J, Aibiki M, et al. . Part 4: advanced life support: 2015 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Circulation. 2015;132(16)(suppl 1):S84-S145. - PubMed
-
- Longstreth WT., Jr Brain resuscitation after cardiopulmonary arrest. Acta Anaesthesiol Belg. 1988;39(3)(suppl 2):115-119. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
