

Extracardiac imaging findings in COVID-19-associated multisystem inflammatory syndrome in children
- PMID: 33433671
- PMCID: PMC7801777
- DOI: 10.1007/s00247-020-04929-1
Extracardiac imaging findings in COVID-19-associated multisystem inflammatory syndrome in children
Abstract
Background: Coronavirus disease 2019 (COVID-19)-associated multisystem inflammatory syndrome in children (MIS-C) is an emerging syndrome that presents with a Kawasaki-like disease and multiorgan damage in children previously exposed to COVID-19.
Objective: To review the extracardiac radiologic findings of MIS-C in a group of children and young adults with a confirmed diagnosis of MIS-C.
Materials and methods: In a retrospective study from April 1, 2020, to July 31, 2020, we reviewed the imaging studies of 47 children and adolescents diagnosed with MIS-C, 25 females (53%) and 22 males (47%), with an average age of 8.4 years (range 1.3-20 years). Forty-five had chest radiographs, 8 had abdominal radiographs, 13 had abdominal US or MRI, 2 had neck US, and 4 had brain MRI.
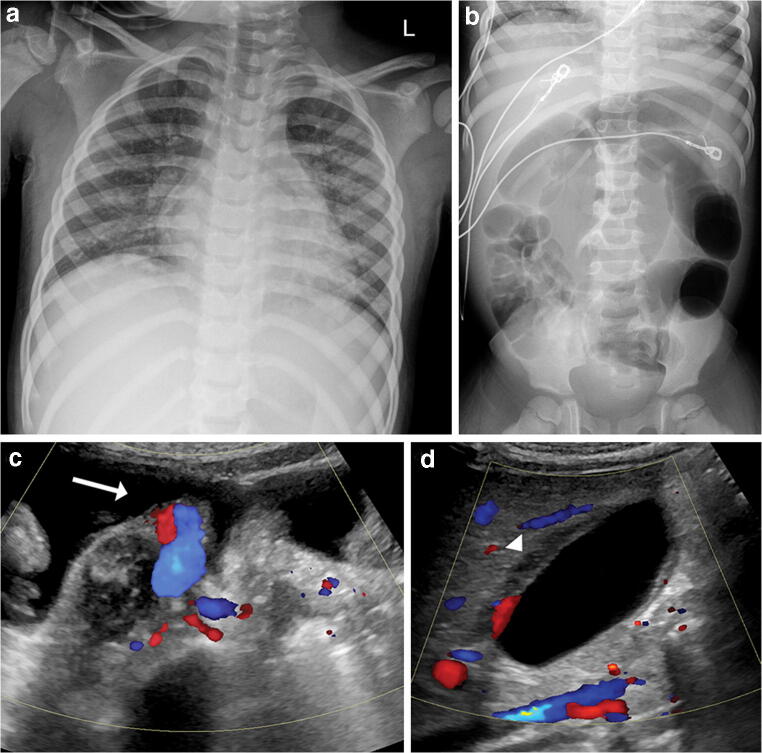
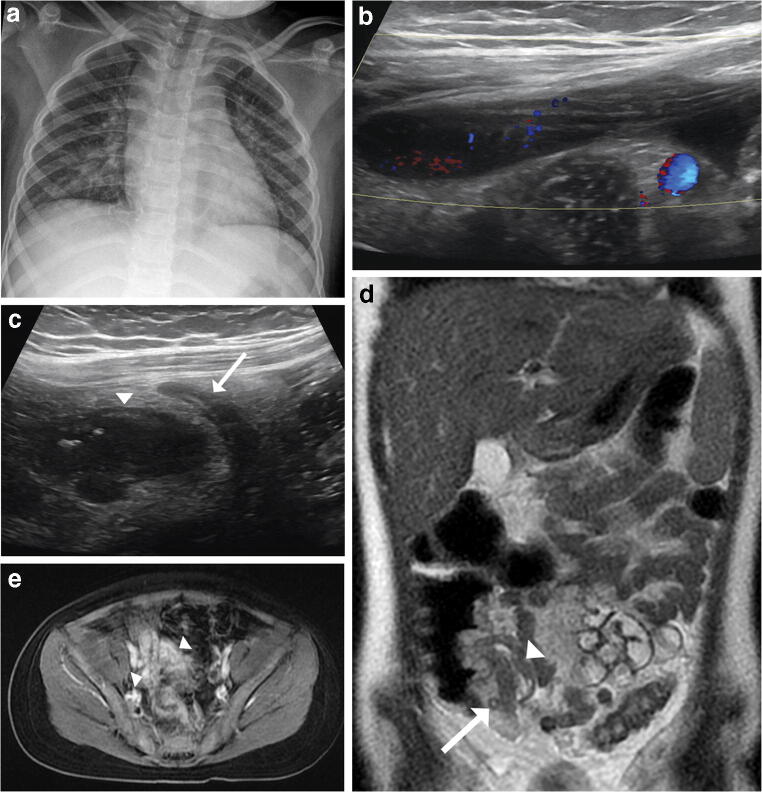
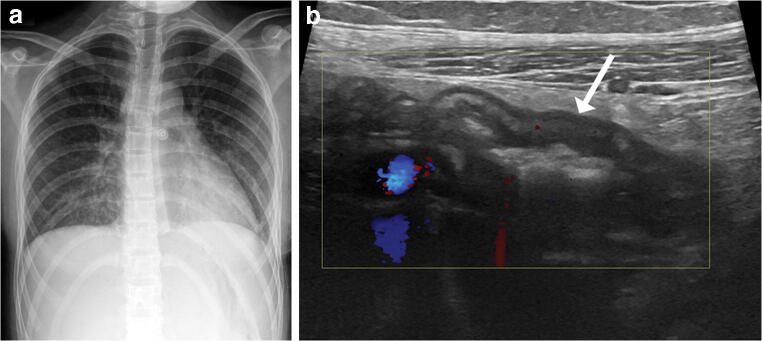
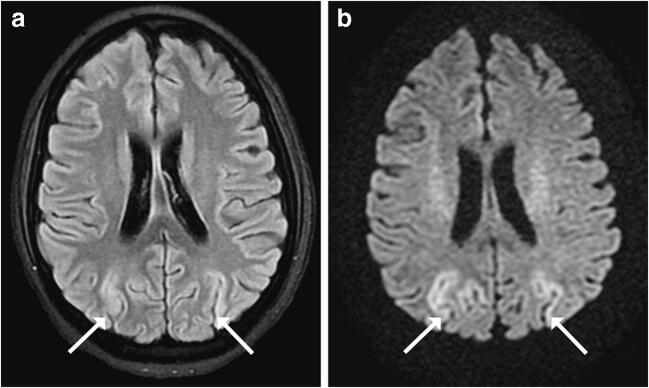
Results: Thirty-seven of 45 (82%) patients with chest radiographs had findings, with pulmonary opacities being the most common finding (n=27, 60%), most often bilateral and diffuse, followed by peribronchial thickening (n=26, 58%). Eight patients had normal chest radiographs. On abdominal imaging, small-volume ascites was the most common finding (n=7, 54%). Other findings included right lower quadrant bowel wall thickening (n=3, 23%), gallbladder wall thickening (n=3, 23%), and cervical (n=2) or abdominal (n=2) lymphadenopathy. Of the four patients with brain MRI, one had bilateral parieto-occipital abnormalities and another papilledema.
Conclusion: The diagnosis of MIS-C and its distinction from other pathologies should be primarily based on clinical presentation and laboratory evidence of inflammation because imaging findings are nonspecific. However, it should be considered in the setting of bilateral diffuse pulmonary opacities, peribronchial thickening, right lower quadrant bowel inflammation or unexplained ascites in a child presenting with Kawasaki-like symptoms and a history of COVID-19 infection or recent COVID-19 exposure.
Keywords: Abdomen; Children; Coronavirus disease 2019; Lungs; Magnetic resonance imaging; Multisystem inflammatory syndrome in children; Radiography; Ultrasound.
Conflict of interest statement
None
Figures

Comment in
-
Imaging in support of the clinical diagnoses of COVID-19 and multisystem inflammatory syndrome in children.Pediatr Radiol. 2021 May;51(5):693-694. doi: 10.1007/s00247-021-04999-9. Epub 2021 Feb 17. Pediatr Radiol. 2021. PMID: 33595703 Free PMC article. No abstract available.
References
-
- CDC Health Alert Network (2020) Multisystem inflammatory syndrome in children (MIS-C) associated with coronavirus disease 2019 (COVID-19). Centers for Disease Control and Prevention website. https://emergency.cdc.gov/han/2020/han00432.asp. Accessed 10 June 2020
-
- Royal College of Paediatrics and Child Health – Health Policy Team (2020) Guidance: paediatric multisystem inflammatory syndrome temporally associated with COVID-19 (PIMS). Royal College of Paediatrics and Child Health website. https://www.rcpch.ac.uk/resources/guidance-paediatric-multisystem-inflam.... Accessed 10 June 2020
-
- Capone C, Subramony A, Sweberg T, et al. Characteristics, cardiac involvement, and outcomes of multisystem inflammatory syndrome of childhood associated with severe acute respiratory syndrome coronavirus 2 infection. J Pediatr. 2020;224:141–145. doi: 10.1016/j.jpeds.2020.06.044. - DOI - PMC - PubMed
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
