

Seroprevalence of SARS-CoV-2 antibodies in over 6000 healthcare workers in Spain
- PMID: 33434269
- PMCID: PMC7928898
- DOI: 10.1093/ije/dyaa277
Seroprevalence of SARS-CoV-2 antibodies in over 6000 healthcare workers in Spain
Abstract
Background: Spain has one of the highest incidences of coronavirus disease 2019 (COVID-19) worldwide, so Spanish health care workers (HCW) are at high risk of exposure. Our objective was to determine severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) antibody seroprevalence amongst HCW and factors associated with seropositivity.
Methods: A cross-sectional study evaluating 6190 workers (97.8% of the total workforce of a healthcare-system of 17 hospitals across four regions in Spain) was carried out between April and June 2020, by measuring immunoglobulin G (IgG)-SARS-CoV-2 antibody titres and related clinical data. Exposure risk was categorized as high (clinical environment; prolonged/direct contact with patients), moderate (clinical environment; non-intense/no patient contact) and low (non-clinical environment).
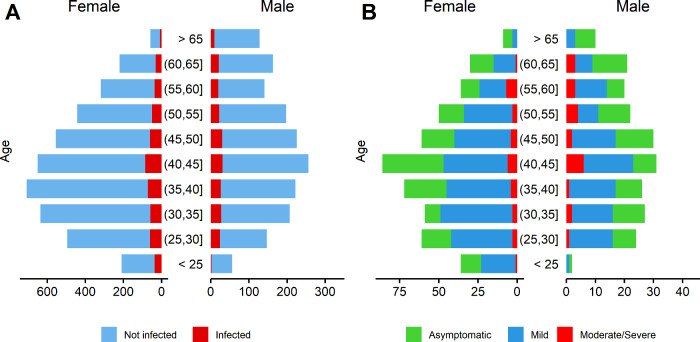
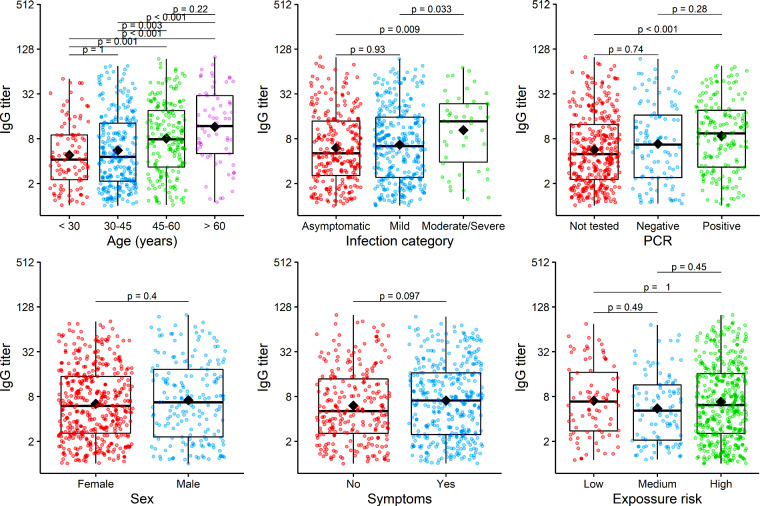
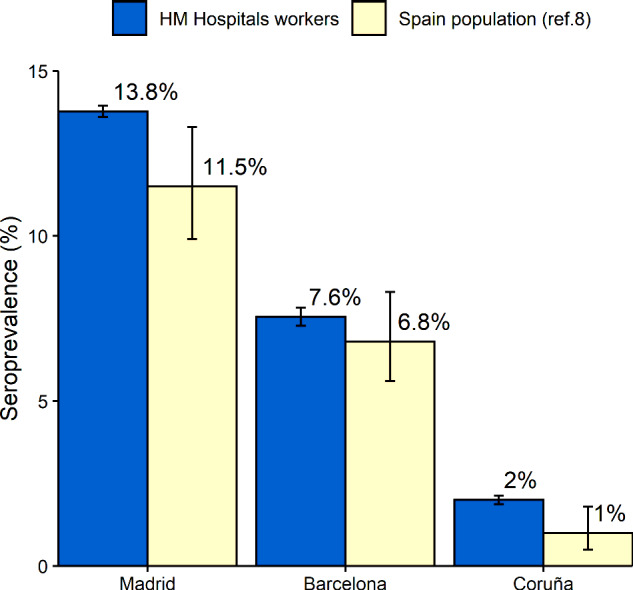
Results: A total of 6038 employees (mean age 43.8 years; 71% female) were included in the final analysis. A total of 662 (11.0%) were seropositive for IgG against SARS-CoV-2 (39.4% asymptomatic). Adding available PCR-testing, 713 (11.8%) employees showed evidence of previous SARS-CoV-2 infection. However, before antibody testing, 482 of them (67%) had no previous diagnosis of SARS-CoV-2-infection. Seroprevalence was higher in high- and moderate-risk exposure (12.1 and 11.4%, respectively) compared with low-grade risk subjects (7.2%), and in Madrid (13.8%) compared with Barcelona (7.6%) and Coruña (2.0%). High-risk [odds ratio (OR): 2.06; 95% confidence interval (CI): 1.63-2.62] and moderate-risk (OR: 1.77; 95% CI: 1.32-2.37) exposures were associated with positive IgG-SARS-CoV-2 antibodies after adjusting for region, age and sex. Higher antibody titres were observed in moderate-severe disease (median antibody-titre: 13.7 AU/mL) compared with mild (6.4 AU/mL) and asymptomatic (5.1 AU/mL) infection, and also in older (>60 years: 11.8 AU/mL) compared with younger (<30 years: 4.2 AU/mL) people.
Conclusions: Seroprevalence of IgG-SARS-CoV-2 antibodies in HCW is a little higher than in the general population and varies depending on regional COVID-19 incidence. The high rates of subclinical and previously undiagnosed infection observed in this study reinforce the utility of antibody screening. An occupational risk for SARS-CoV-2 infection related to working in a clinical environment was demonstrated in this HCW cohort.
Keywords: COVID-19; SARS-CoV-2; healthcare workers; seroprevalence.
© The Author(s) 2021; all rights reserved. Published by Oxford University Press on behalf of the International Epidemiological Association.
Figures
References
-
- World Health Organization (WHO). Coronavirus disease (COVID-19). https://www.who.int/emergencies/diseases/novel-coronavirus-2019
-
- Análisis de los casos de COVID-19 en personal sanitario notificados a la red nacional de vigilancia epidemiológica (RENAVE) hasta el 10 de mayo en España. Informe a 29 de mayo de 2020. Equipo Covid-19. RENAVE. Centro Nacional de Epidemiología CNM. Instituto de Salud Carlos III. https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/...
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
